Download
1 / 43
430 likes | 461 Views
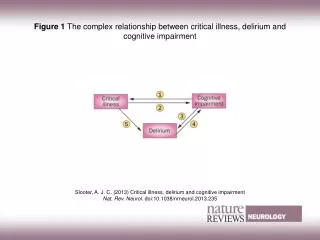
Explore the role of imaging in diagnosing dementia and cognitive impairment, including challenges and advancements. Learn about Alzheimer's Disease, Frontotemporal Dementia, and imaging techniques like MRI and PET scans. ###

E N D
Imaging in dementia / cognitive impairment Dr Richard Perry Consultant Neurologist Imperial College Healthcare NHS Trust UK AMY00125 February 2015
Overview • Diagnosing dementia versus diagnosing cause of dementia • AD, FTD, MCI, prodromal and pre-clinical AD • Two phase approach • Is there a brain disease? • What is the cause of the brain disease • Diagnosis of Alzheimer’s Disease • How accurate is current diagnosis • What are the challenges? • MRI, FDG PET, Neuropsych, CSF, amyloid imaging • Frontotemporal Dementia
Diagnosing dementia vs diagnosing Alzheimer’s Disease • It is relatively straightforward to diagnose dementia in an elderly patients with typical symptoms and a moderate stage of dementia • Alzheimer’s Disease – less straightforward if: • Earlier in course of condition • Atypical presentation • Young Onset • Multiple pathologies
Role of imaging in dementia diagnosis NICE guidance: Structural imaging should be used in the assessment of people with suspected dementia to exclude other cerebral pathologies and to help establish the subtype diagnosis. Magnetic resonance imaging (MRI) is the preferred modality to assist with early diagnosis and detect subcortical vascular changes, although computed tomography (CT) scanning could be used.
Beyond diagnosing dementia • The key questions that clinicians have to address are: • Does this patient have dementia? • If yes, is it a typical sub-type presentation? • If no, does the patient have objective evidence of impaired cognition? • If yes to this, does this patient have symptoms that are secondary to a brain disease? • If yes, what is the brain disease? • If no, is there a definite cause of the symptoms?
Pathology of Alzheimer’s Disease β Amyloid – plaques, extracellular Tau – abnormally hyperphosphorylated tau → neurofibrillary tangles Plus neuronal and synaptic loss
When does Alzheimer’s Disease start? Fibrillar amyloid deposition as measured by PET imaging in carriers of autosomal dominant AD mutations
Alzheimer’s disease- diagnosisNational Institute of Neurologic and Communicative Disorders and Stroke – Alzheimer’s Disease and Related Disorders Association • Definite AD – clinical diagnosis with histopathological confirmation • Probable AD – typical clinical picture without histological confirmation • Sensitivity and specificity ca 80% • Usually made with help of blood tests, neuroimaging and neuropsychological assessment
Alzheimer’s disease without dementia?Mild Cognitive Impairment (MCI) Cognitive decline greater that that expected for age and education level but does not interfere with ADLs Can be seen as an entity with high risk for conversion to dementia
MCI not due to Alzheimer’s Disease • Depression and anxiety • Drugs • E.g beta blockers, anticholinergics - tricyclics, antiemetics, antispasmodics, antiarrythmics, analgesics • Cerebrovascular disease • Risk factors • Cognitive slowing, slowing of gait (wide-based) • Other neurodegenerative diseases • Dementia with Lewy Bodies, FrontotemporalDementia • Ageing? Argyrophyllic grain disease?
Alzheimer’s DiseaseTypical and atypical presentations • 40 % of EOAD may be non-amnestic • 10% LOAD non-amnestic • Posterior Cortical Atrophy • Progressive aphasia • Logopenic aphasia • Progressive non-fluent aphasia • Dysexecutive / frontal AD Atypical presentations
Investigations in Alzheimer’s Disease diagnosis • Neuropsychology • Structural brain imaging • FDG PET imaging • CSF
Diagnostics: Neuropsychology • Advantages • Low cost of technology • Portable • Disadvantages • Time consuming • Variance in population • Affected by culture and education • Lacks specificity and sensitivity e.g. depression or prodromal AD
Diagnostics - CSF • Advantages • Pathology specific for tau and abeta • Sensitive • Disadvantages • Invasive • Dependent on processing and assay stability
How does imaging answer our clinical questions? • Markers of neuronal loss • MRI • Hippocampal atrophy • Focal atrophy • White matter hyperintensities - ? Vascular disease • FDG – PET • Pathology sensitive imaging • Amyloid PET imaging
Diagnostics – structural imaging • Advantages • Marker of neuronal loss • Patterns of atrophy • Exclude other pathologies e.g NPH, vascular changes • Not confined by educational / cultural factors • Quick, safe • Disadvantages • Not pathology specific • Insensitive in earliest disease • Dependent on experience of radiologist
White matter hyperintensities and cognitive impairmentCheese is yellow, the moon is yellow…. Cognitive impairment + WMH on imaging report ≠ vascular dementia Usually co-existent degenerative disease that is responsible for the cognitive impairment First symptoms and course of disease important e.g. early episodic memory impairment with progressive cognitive impairment and lack of neurological signs Look for gait disorder
MRI and hippocampal atrophy • Definitely abnormal and reported as such is helpful • Definitely abnormal and reported as normal is not helpful • Possibly abnormal and reported as possibly abnormal is not very helpful • Normal hippocampi does not exclude AD
MRI and focal atrophy Semantic dementia Posterior Cortical Atrophy bvFTD • Hippocampal atrophy – biomarker of neuronal degeneration in MCI secondary to AD diagnosis • Dependent on skill of radiologist • Visual rating scales • Quantitative analysis available
Investigations and cascade of events in neurodegenerative disease (AD)Towards pathology sensitive investigations
Developing PET ligands for amyloid- pathology sensitive investigation • PIB Klunk et al 2004 • Pittsburgh Compound B, collaboration with Uppsala • High affinity for fibrillar amyloid • Short half life – need to be near a cyclotron and radiochemistry lab • !8 Fluro compounds developed Nordberg, A. et al.(2010) The use of PET in Alzheimer disease Nat. Rev. Neurol. doi:10.1038/nrneurol.2009.217
Florbetapir - Amyvid • Originally developed as AV-45 by Avid radiopharmaceuticals • Detection of amyloid plaques • Half life 110 minutes • Uptake 30 minutes • 10 minute PET scan • Result positive or negative • Grey scale • Pivotal pathological study, Clarke et al Lancet Neurol 2012 • 59 end of life patients, sensitivity 92% and specificity 100 %
Florbetapir - Amyvid • FDA approved 2012. Licensed in patients with cognitive impairment who are being evaluated for Alzheimers disease (AD) and other causes of cognitive impairment • UK guidelines recommend use by dementia experts in cases of possible AD where previous Ix inconclusive and where diagnostic clarity changes management • A scan for amyloid plaques, not a scan for Alzheimer’s Disease • Negative scan – highly unlikely that cognitive impairment due to AD pathology
Our approach to amyloid PET imaging • Through a Multidisciplinary Team • Neuroradiologists and nuclear medicine physicians with neurologists, psychiatrists, geriatricians • Discuss the case of each request and review MRI imaging • Review PET imaging post scan
Case 1 - RD • 58 yr old district nurse • 18/12 Hx of memory problems and organisational difficulties at work • Local memory clinic MMSE 30/30, ACE-R 97/100 • MRI normal • SPECT reported as showing medial temporal hypoperfusion • Given diagnosis of AD and started on donepezil
Case 1 - RD • Referred for second opinion • Husband felt that memory OK • Daughter reported her as repetitive and more noticeable symptoms over last year • ACE -96, MMSE 28 – one point on orientation and one on memory
Case 2 - SN 2 yr Hx of decreasing verbal output Apathy and passivity EEG showed L frontal slow wave activity Diagnosis – Frontotemporal Dementia
Case 3 - BS • 49 yr old with progressive language impairment 2 yrs • Non-fluent aphasia • Mild apraxia CSF tau level = 1004 CSF abeta level = 379 Genetic testing showed PS-1 mutation Diagnosis – Familial Alzheimer’s Disease
Case 2 -VW • 63 yr old woman – Editor for Mensa magazine • 18/12 Hx of memory problems and oranisational difficulties • Collects things, less empathic • Likes eating biscuits • Non-fluent aphasia • Stimulus bound behaviour • Had MRI imaging, FDG PET imaging and neuropsych before referral
Case 3 - LC • Progressive memory deficits corroborated by husband • Previous Hx of ME, anxiety, and depression • MMSE 26/30 • Neuropsych suggest a specific mild deficit in delayed recall of information, particularly for visual information.Given the multiple factors involved, it is not clear what may be contributing to the deficit in recall of information observed. • MRI unremarkable
Case 4 - DT • Walking memory speech • Emotional change after loosing son in RTA 8 yrs previously • Decreased motivation • Muddled • Not really forgetful • MMSE 17/20 2014, and 22/30 in 2011 • Neuropsych showed reduced encoding but normal delayed recall, poor attentional and executive dysfunction – felt to be not consistent with AD but suggestive of frontal-subcortical dementia • Diagnosed VaD and depression
Case 5 • 49 year old woman • 18/ 12 progressive loss of memory, visuospatial function, executive function. • Myoclonic jerks • No FH • MMSE 22/30 • Genetics negative for PS-1, PS-2, and APP
Amyloid imaging in Young Onset Dementia • 80 early onset dementia subjects • Amyloid PET discordant with clinical Dx in 25% • Changes in management in 50% of cases Zwan MD AAIC 2014
Which patients are suitable for amyloid imaging? • It’s a new area, so we are still calibrating • Currently, we are focusing on: • Younger patients – less probability of ‘false positive’ • Atypical AD presentations – e.g. PCA, Progressive Aphasia • AD / FTD differentiation • MCI if clarification helpful • Multiple possible causes of cognitive impairment e.g depression / vascular / medical co-morbities / Normal Pressure Hydrocephalus
Before and after an amyloid scan Before • Open discussion with patient and family about what scan is for • Discussion about what they want to know • Discussion about what a positive scan or negative scan would mean in their own situation
After an amyloid scan • Negative scan • Was scan good quality and a clear read? • Cognitive impairment highly unlikely to be due to Alzheimer’s Disease • Caution in > 80’s • What is causing the cognitive impairment? • Follow up • Positive scan • Positive for amyloid plaque, may be supportive of a diagnosis of Alzheimer’s Disease • Interpretation needs caution and context • Age (? Apo E status) • Cognitive deficits • Possibility of dual pathology • Evidence of neuronal loss • May lay ground for working diagnosis and management plan
Conclusions • Investigations support clinical diagnosis • Investigations can be thought of as biomarkers that are: • Supportive of neurodegeneration and / or • Pathology or disease specific • Familiarity with Ix important and important to review actual pictures • Amyloid imaging e.g. Amyvidnow available for use within guidelines
Conclusions Detection of amyloid is not a diagnosis of AD Amyloid PET results must be interpreted in the context of a comprehensive clinical evaluation – see MDT with neuroradiology Negative scan effectively excludes amyloid pathology Has greatest utility in young onset dementia, atypical presentations, differentiating from AD from FTD, and in cases where there are multiple pathologies, e.g. depression, vascular