Download
1 / 2
20 likes | 242 Views
This patient presented following a trauma to the maxillary anterior region. She had suffered lateral luxation injuries to teeth 21 and 22, only avoiding complete avulsion of the teeth due to the presence of the orthodontic maxillary archwire .

E N D
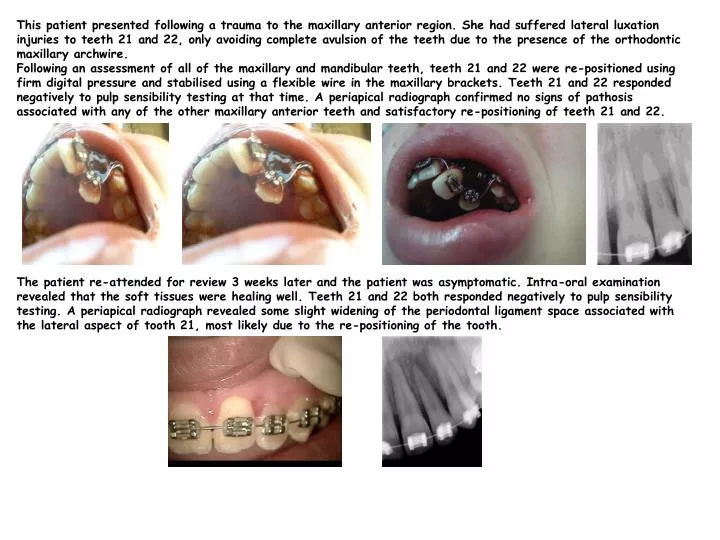
This patient presented following a trauma to the maxillary anterior region. She had suffered lateral luxation injuries to teeth 21 and 22, only avoiding complete avulsion of the teeth due to the presence of the orthodontic maxillary archwire. Following an assessment of all of the maxillary and mandibular teeth, teeth 21 and 22 were re-positioned using firm digital pressure and stabilised using a flexible wire in the maxillary brackets. Teeth 21 and 22 responded negatively to pulp sensibility testing at that time. A periapical radiograph confirmed no signs of pathosis associated with any of the other maxillary anterior teeth and satisfactory re-positioning of teeth 21 and 22. The patient re-attended for review 3 weeks later and the patient was asymptomatic. Intra-oral examination revealed that the soft tissues were healing well. Teeth 21 and 22 both responded negatively to pulp sensibility testing. A periapical radiograph revealed some slight widening of the periodontal ligament space associated with the lateral aspect of tooth 21, most likely due to the re-positioning of the tooth.
The patient returned for review six weeks later at which time the teeth still gave negative responses to pulp testing. However, at the 4 month review appointment, tooth 22 gave a faint response to cold testing and a positive response to electrical testing. At the 18 month review appointment, the patient was again asymptomatic. There were no signs of infection or inflammation associated with the maxillary anterior teeth. However, both teeth 21 and 22 responded positively to electrical testing. A periapical radiograph revealed that there was pulpal obliteration of tooth 22 and blunting of the apices associated with both teeth. There were, however, no signs of apical pathosis. Discussion This case reinforces the concept that prompt and conservative management of trauma cases is the most effective approach. The outcome following a severe traumatic injury such as this is dependent, of course on the extent of the injury but also on the correct and efficient re-positioning of the luxated teeth. This was faciltated by the presence of the maxillary orthodontic brackets. Regular review of these cases is important in order to monitor for signs of pulpal necrosis and infection or possibly infection-related inflammatory root resorption. In this case, although there was pulp canal obliteration of tooth 22 there were no associated signs of infection or inflammation and so a decision was taken to monitor tooth 22. These teeth should be followed up in case of the development of pulpal necrosis and infection visible by the presence of peri-apical radiolucency. About 1% of pulp canal obliteration cases are associated with the development of pulpal necrosis and infection. Andreasen FM, Vestergaard Pedersen B. Prognosis of luxated permanent teeth – the development of pulp necrosis. Endod Dent Traumatol 1985; 1: 207–220. Andreasen FM, Zhijie Y, Thomsen BL, Anderson PK. Occurrence of pulp canal obliteration after luxation in the permanent dentition. Endod Dent Traumatol 1987; 3: 103–115. Elena C, Ferrazzini P, von Arx T. Pulp and periodontal healing of laterally luxated permanent teeth: results after 4 years. Dent Traumatol 2008; 24: 658-662.