Download
1 / 33
330 likes | 459 Views
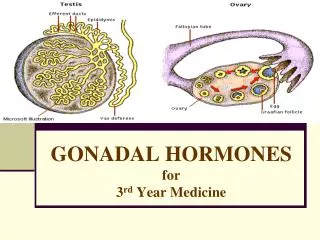
Endocrine diseases. Genital tract diseases. Lecture on pathomorphology for the 3-rd year students By T.G.Filonenko. Diabetes mellitus. Diabetes mellitus is a metabolic disorder characterized by hyperglycemia. I. Primary Type I, also known as insulin-dependent diabetes mellitus (IDDM)

E N D
Endocrine diseases. Genital tract diseases. Lecture on pathomorphology for the 3-rd year students By T.G.Filonenko
Diabetes mellitus Diabetes mellitus is a metabolic disorder characterized by hyperglycemia
I. Primary Type I, also known as insulin-dependent diabetes mellitus (IDDM) Type II, or non-insulin-dependent diabetes mellitus (NIDDM) Impaired glucose tolerance Gestational diabetes II. Secondary Pancreatic diseases (Chronic pancreatitis, Hemochromatosis, Cystic fibrosis, Tumors of pancreas) Endocrine disorders (Cushing disease, Acromagaly, Pheochromocytoma) Genetic disease (Glycogen storage disease, Down syndrome) Drug-induced (Diuretics, Psychoactive drugs Classification of Diabetes mellitus
Type I(IDDM) Type II(NIDDM)
Complications of DM nodular glomerulosclerosis Glaucoma with excavation of the optic cup budding cells with Candida albicans on PAS stain in the renal pelvis
Islet cell adenoma Insulinoma
A. Graves diseaseis an autoimmune disorder caused by antibodies to the TSH receptor on follicular cells. Follicles are lined by cells that show signs of hyperfunction, and the stroma contains lymphoid follicles. B.Hashimoto thyroiditisis an autoimmune disease of unknown etiology. The thyroid is diffusely infiltrated with lymphocytes. A part of the thyroid is destroyed, and many follicles are lined by Hurthle cells. C. De Quervain (subacute) thyroiditis(orgiant cell or granulomatous thyroiditis) is characterized by a sudden painful enlargement of the thyroid. It is presumed to be of viral origin. The rupture of follicles is associated with an inflammatory response that includes macrophages and giant cells. D.Riedel thyroiditisis a chronic fibrosing process in which dense fibrous tissue replaces the damaged thyroid follicles. There are no antithyroid antibodies in this disease. The thyroid follicles have been replaced by fibrous tissue. Thyroiditis
Graves disease Note the clear vacuoles in the colloid next to the epithelium where the increased activity of the epithelium to produce increased thyroid hormone has led to scalloping out of the colloid.
Hashimoto thyroiditis lymphoid follicle The pink Hürthle cells atrophy
De Quervain (subacute) thyroiditis also known as giant cell or granulomatous thyroiditis the foreign body giant cells with destruction of thyroid follicles
Papillary carcinoma psammoma body
Medullary carcinoma of the thyroid amyloid
Goiter The follicles are irregularly enlarged, with flattened epithelium
THE NORMAL MENSTRUAL CYCLE normal proliferative endometrium early secretory endometrium normal secretory phase endometrium
The causes uterine bleeding • complication of pregnancy (ectopic pregnancy, miscarriage, trophoblastic disease) • submucosal leiomyoma (interferes with the development of the endometrium) • endometrial polyp (abnormal benign patch of endometrium) • endometrial hyperplasia • cancer • "dysfunctional uterine bleeding", i.e., some problem with the hormonal symphony; this is the most common
Causes of Dysfunctional uterine bleeding • Anovulatory cycles • A granulosa and/or theca tumor in an ovary producing estrogens and/or progesterone • Endocrine disease elsewhere • Massive obesity (too much estrogen being converted) • Too little body fat (too little estrogen being converted) • Severe chronic disease • Inadequate luteal phase • Persistent luteal phase
ADENOMYOSIS ("endometriosis interna") endometrial glands and stroma in the myometrium
The gross appearance of endometriosis Minor lesions look like powder burns under the serosal surface Repeated hemorrhage in a cystic space in the ovary (so-called "chocolate cyst")
To make the diagnosis, the pathologist must find two of three: • endometrial glands • endometrial stroma • hemosiderin (from the bleeding) small cluster of endometrial glands and stroma with hemorrhage in the surface of the fallopian tube Hemosiderin in the wall of "chocolate cysts" Endometrial glands and stroma are seen at high magnification in the wall of the colon.
submucosal, intramural, and subserosal leiomyomata of the uterus Endometrial polyp
ENDOMETRIAL HYPERPLASIA Endometrial hyperplasia usually results with conditions of prolonged estrogen excess and can lead to metrorrhagia (uterine bleeding at irregular intervals), menorrhagia (excessive bleeding with menstrual periods), or menometrorrhagia.
Simple hyperplasia ("cystic • hyperplasia", "mild hyperplasias") • features: • glands of very uneven sizes • cystically dilated glands • no anaplasia • no extra cancer risk
Complexhyperplasia • ("complex / adenomatous • hyperplasia without atypia") • crowded glands • irregularly-shaped glands • no anaplasia • about 5% risk of turning • into adenocarcinoma
Atypical hyperplasia • ("higher grade hyperplasia") • crowded, • irregular glands, • "budding", • but there is still stroma between them • anaplasia (bizarre cells, • some piling up or "tufting") • about 25% risk of • turning into adenocarcinoma
The placenta has invaded far enough through the wall of the tube to make it rupture, with massive internal bleeding. • The expanding mass passes back out through the fimbriated end of the oviduct ("tubal abortion"). • The placenta comes off the wall of the tube, causing heavy bleeding. • Or the baby can simply die, and the whole gestation gets reabsorbed. Rarely the baby calcifies (a "lithopedion", or stone child). Location: the oviduct, though ovary, peritoneum, uterine cornua and intraperitoneal pregnancy Best-known cause is old pelvic inflammatory disease, scarring from endometriosis, previous laparotomy
tubal epithelium Rupture site and chorionic villi Blood clot and chorionic villi recovered outside of the tube following rupture of an ectopic pregnancy.
Hydatidiform mole Molar pregnancies are uncommon and occur when there is fertilization of an ovum by a sperm but loss of maternal chromosomes, leaving a 46XX karyotype composed only of paternal chromosomes, enough to form a placenta, but not a fetus. The result is a mass of tissue with grape-like swollen villi.
Partial mole that occurs when two sperms fertilize a single ovum. The result is triploidy (69 XXY). Only some of the villi are grape- like, and a fetus can be present, but rarely survives past 15 weeks.