Download
1 / 16
230 likes | 864 Views
Stomach Anatomy and Pathology . Week 4- Feeling Tired Skye Poulton . The stomach is Intraperitoneal Lesser omentum has superior attachment to liver by lesser curvature Greater omentum suspended from greater curvature of stomach and loops back up to attach to transverse colon.

E N D
Stomach Anatomy and Pathology Week 4- Feeling Tired Skye Poulton
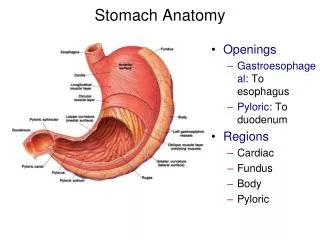
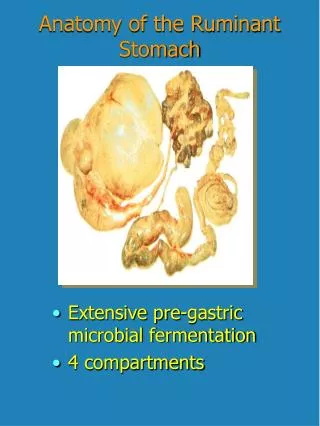
The stomach is Intraperitoneal • Lesser omentum has superior attachment to liver by lesser curvature • Greater omentum suspended from greater curvature of stomach and loops back up to attach to transverse colon
Has four regions • Cardia • Fundus • Body • Pyloric
Blood Supply • The rich arterial supply of the stomach arises from the celiac trunk and its branches • Most blood is supplied by anastomoses formed along the lesser curvature by the right and left gastric arteries, and along the greater curvature by the right and left gastro-omental (gastroepiploic) arteries. • The fundus and upper body receive blood from the short and posterior gastric arteries. • The veins of the stomach parallel the arteries in position and course
Gastric Innervation • Receives Parasympathetic innervations from medulla via vagus nerves • Receives Sympathetic innervations from celiac ganglia arising from T5 – T9 Lymphatic Drainage • mainly to the gastric lymph nodes, pancreaticosplenic lymph nodes, pyloric lymph nodes and pancreatic-oduodenal lymph nodes • then drainage accompany the large arteries to the celiac lymph nodes
Histology • Glandular Epithelium • Gastric Pits and Glands • Extra layer in muscularis Propria- Inner Oblique Layer
Structure of Glands • Surface/Neck mucous cells- secrete protective bicarbonate ions • ParietalCells- most numerous in the isthmus of the glands, secrete gastric acid (HCL) as well as intrinsic factor. • Chief, peptic or zymogenic cells- located towards the bases of the gastric glands. Secrete gastric lipase and pepsinogen. • Neuroendocrine cells- part of the diffuse neuroendocrine system, secrete serotonin and other hormones • Stem cells- divide continuously to replace all other types of cell in the glands. Not easily but become very prominent with plentiful mitotic figures after damage to the mucosa has occurred, e.g. after an episode of gastritis. ie. important histopathology feature
Stomach- Pathologies Acute Gastritis - a transient mucosal inflammatory process that may be asymptomatic or cause variable degrees of epigastric pain, nausea, and vomiting. In more severe cases there may be mucosal erosion, ulceration, hemorrhage, hematemesis, melena, or, rarely, massive blood loss. Pathophysiology: The gastric lumen is strongly acidic with pH close to 1. This harsh environment contributes to digestion but also has the potential to damage the gastric mucosa, if any of the protective mechanisms that have evolved are disrupted. • Reduced mucin synthesis in the elderly • NSAIDs prevents synthesis of prostaglandins, which enhance bicarbonate secretion, inhibit acid secretion, promote mucin synthesis, and increase vascular perfusion • urease-secreting H. pylori inhibitions gastric bicarbonate transporters by ammonium ions. • Direct cellular injury due to excessive alcohol consumption, NSAIDs, radiation therapy, and chemotherapy. This diagram illustrates the progression from more mild forms of injury to ulceration that may occur with acute or chronic gastritis
Chronic Gastritis • In contrast to acute gastritis, the symptoms are typically less severe but more persistent. • The most common cause of chronic gastritis is infection with H. Pylori. Although the mechanism is incompletely defined, it is clear that infection results in increased acid production and disruption of normal gastric and duodenal protective mechanisms. • Four features are linked to H. pylori virulence: • Flagella, which allow the bacteria to be motile in viscous mucus • Urease, which generates ammonia from endogenous urea and thereby elevates local gastric pH • Adhesins that enhance their bacterial adherence to surface foveolar cells • Toxins, such as cytotoxin-associated gene A (CagA), that may be involved in ulcer or cancer development by poorly defined mechanisms • Other chronic irritants, including psychologic stress, caffeine, alcohol, and tobacco • Peptic Ulcer Diseases- chronic reoccurring lesions • complication of chronic Gastritis: the imbalances of mucosal defenses and damaging forces
Autoimmune gastritis • the most common cause of atrophic gastritis, and the most common form of chronic gastritis in patients without H. pylori infection. Autoimmune gastritis is characterized by: • Antibodies to parietal cells and intrinsic factor that can be detected in serum and gastric secretions • Reduced serum pepsinogen I concentration • Antral endocrine cell hyperplasia • Vitamin B12 deficiency • Defective gastric acid secretion Pathogenesis: believed that CD4+ T cells directed against parietal cell components, including the H+,K+-ATPase, are the principal agents of injury. This is supported by the observation that transfer of H+,K+-ATPase-reactive CD4+ T cells into mice results in gastritis and production of autoantibodies. • Loss of parietal cells absence of acid production gastrin release hypergastrinemia and hyperplasia of antral gastrin-producing G cells. • Loss of parietal cells lack of intrinsic factor B12 deficiency and a slow-onset megaloblastic anaemia (pernicious anaemia). • Gastric Gland destruction consequential chief cell destruction reduced serum pepsinogen concentration
Atrophy, Metaplasia and Dysplasia • Long-standing chronic gastritis that involves the body and fundus may ultimately lead to significant loss of parietal cell mass. This atrophy may be associated with intestinal metaplasia, recognized by the presence of goblet cells, and is strongly associated with increased risk of gastric adenocarcinoma. • Chronic gastritis exposes the epithelium to inflammation-related free radical damage and proliferative stimuli. Over time this can lead to the accumulation of genetic alterations that result in carcinoma. Pre-invasive in situ lesions can be recognized histologically as dysplasia. • Dysplasia- in the form of Polyps, and adenomas almost always occur on a background of chronic gastritis with atrophy and intestinal metaplasia.
Adenocarcinoma • Adenocarcinoma is the most common malignancy of the stomach, comprising over 90% of all gastric cancers. • Unfortunately early symptoms resemble those of chronic gastritis. • Although specific sequences of events have not been defined, it is clear that chronic inflammation promotes neoplastic progression. • While the majority of gastric cancers are not hereditary, many genetic mutations have been identified • mutations in CDH1, and the subsequent loss of E-cadherin function, a protein that contributes to epithelial intercellular adhesion, is a key step in the development of diffuse gastric cancer. • BRCA2 mutations are at increased risk of developing diffuse gastric cancer. • several genes including TGFβRII, BAX, IGFRII, and p16/INK4a have also been described in sporadic intestinal-type gastric cancer. • Genetic variants of pro-inflammatory and immune response genes, including those that encode IL-1β, TNF, IL-10, IL-8, and Toll-like receptor 4 (TLR4), are associated with elevated risk of gastric cancer when accompanied by H. pylori infection • p53 mutations are present in the majority of sporadic gastric cancers of both histologic types.
Hypertrophic Gastropathies • Hypertrophic gastropathies are uncommon diseases characterized by giant cerebriform enlargement of the rugal folds due to epithelial hyperplasia without inflammation. • As might be expected, the hypertrophic gastropathies are linked to excessive growth factor release. The two most well-understood examples: • Zollinger-Ellison syndrome is caused by gastrin-secreting tumors, gastrinomas, that are most commonly found in the small intestine or pancreas. • Ménétrier disease is a rare disorder caused by excessive secretion of transforming growth factorα (TGF-α)
Vitamin B12 has no appreciable toxicity level………. So no risk to her health of continuing B12 injections.
References • Kumar. V., et L. (2010). Robbins and Cotran pathologic basis of disease, 8th Edn. Philadelphia: Saunders/Elsevier. • Moore, K.L. & Agur, A.M.R. (2007). Essential clinical anatomy. 3rd edn. Baltimore: Lippincott Williams & Wilkins. • Young, B. et al. (2006). Wheater's functional histology : A text and colour atlas. 5th edn. New York: Churchill Livingstone.