Download
1 / 60
640 likes | 812 Views
Anatomy of stomach and its relations. By Praveen Panicker. STOMACH(ventriculus/gaster). Most dilated part of GIT Occupies in the epigastric, umbilical &left hypochondral areas

E N D
Anatomy of stomach and its relations • By Praveen Panicker
STOMACH(ventriculus/gaster) • Most dilated part of GIT • Occupies in the epigastric, umbilical &left hypochondral areas • Occupying a recess bounded by upper abdominal viscera, completed above& anterolateraly by anterior abd wall &diaphragm
Stomach • Roughly J Shaped at rest • Size and Shape varies with • a) Volume of food or fluid it contains • b) Position of body • c) Phase of respiration • High and transverse in obese and short persons • Elongated in thin persons
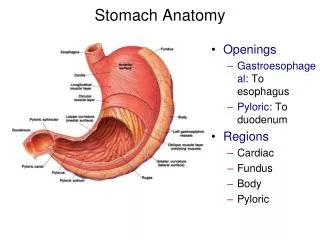
Mean capacity 30ml at birth 1000ml at puberty 1500ml at adult 2 OPENINGS 2SURFACES 2BORDERS
Gastric orifices • Cardiac orifices • Situated to the left of midline behind 7th costal cartilage 2.5cm from its sternal junction at the level of T11 • 10 cm from ant abd wall • 40 cm from incisor teeth
Pyloric orifice • Can be identified by prepyloric vein crossing its anterior surface vertically • 1.2cm to right of midline in trans pyloric plane provided the body is supine & stomach is empty
Gastric curvatures Lesser curvature • Extends b/w cardiac & pyloric orifice forming right border • Incisura angularis is a notch in the most dependent part ,its position varies with gastric distension • Gives attachment to lesser omentum
Greater curvature • 4 to 5 times longer than lesser curvature • Starts at cardiac incisure • Arches upwards & postero laterally & to Lt • Highest convexity is fundus Lt 5th ICS • Finally turns right to end at the pylorus Attachments • Lt of fundus & adjoining body - gastrosplenic lig. • Beyond this - greater omentum
Gastric surfaces Antero superiorPostero inferior • Antero superior surface Lt part of this surface is posterior to Lt costal margin & in contact with diaphragm. It is related to costal attachments of upper fibers of transverse abdominis which separate it from7th to 9th costal margin
Upper &Left part of this surface becomes postero lateral & is in contact with spleen’s gastric surface • Rt half of this surface is related to Lt & quadrate lobe of liver & ant abd wall • Whole of the surface is covered by peritoneum. • part of greater sac separate it from above structures
Related to STOMACH BED diaphragm Lt suprarenal gland upper part of front of left kidney splenic artery anterior pancreatic surface colic flexure together with transverse mesocolon Postero inferior surface
This surface is also covered by peritoneum except near the cardiac orifice where a small triangular area contacts diaphragmatic crus
A large globular Lt part & a narrow tubular Rt part INTERIOR OF STOMACH
Gastric micro structure • Mucosa • Sub mucosa • Muscularis externa • Serosa • Mucosa • Thick, smooth surface, velvetty • Reddish brown to pink in colour
In contracted state mucosa is folded to form RUGAE. They are Longitudinal & more marked towards pyloric & greater curvature Actually they are large folds in sub mucosal connective tissue Obliterated when stomach is distended
MUCOSA • Epithelium • Lamina propia • Muscularis mucosa
Epithelium Appears as honey combed due to small gastric pits (foveola). Base of gastric pits (foveola) receives gastric glands which extend deep into lam propria Epithelium simple columnar mucous cells
Principal Found In body & fundus Cardiac glands Situated near the cardia Pyloric glands numerous mucous & entero endocrine cells predominate Gastric glands cardiac Principal pyloric
Principal • Highly differentiated • Found In body & fundus Are made of different types of cells Chief Parietal Mucous Stem Entero endocrine
Cardiac glands • Situated near the cardia • Mucous secreting cells predominate Pyloric glands • numerous mucous & entero endocrine cells predominate
Lamina propria Found in b/w the glands Contain gastric follicles which are aggregations of lymphoid tissue A periglandular vascular plexus is also present
Muscularis mucosa • Inner circular • Outer longitudinal • Ext circular in some places • Sub mucosa • Loose connective tissue • Collagen, elastin,sub mucosal plexus of stomach
Oblique fibres Circular longitudinal Muscularis externaFrom within outwards layers are
Oblique fibres Limited to gastric body Most developed near the cardiac orifice Circular fibres Form a uniform layer external to oblique fibres At the pylorus form annular pyloric sphincter
Longitudinal fibres • Arranged in 2 groups • 1st set radiates from cardiac orifice, best developed along the curvatures • 2nd set commence in the body, passes to right, some fibres pass to duodenum, deeper fibres interlace with pyloric sphincter • Muscle action upper region of stomach forms an area of storage, lower region has a pump like axn mixing & delivering the contents to duodenum
Left gastric artery Rt gastric artery Lt & Rt gastro epiploic artery Short gastric artery Gastric vessels
These form anastomosis in all layers, forming sub serosal, intramuscular & sub mucosal plexus ;from these anterior & posterior branches arise • Mucosal arteries usually arise from sub mucosal plexus. But along the curvatures they arise directly from sub serosal arteries without anastomosing with other plexus. So that these are more vulnerable to ischemic injury
pyloric region is supplied by pyloric arteries (br of rt gastric & gastroepiploic) where they form a submucosal plexus. They also anstomose with Duodenal & gastric arteries • Arterioles from Submucosal arterial plexus penetrate the mucosa & branch to form capillary beds which drain to sub mucosal venous plexus
This rich lumen directed blood flow enablesHCO3- generated basally by the parietal cells as a counterpart of their secretion of acid to be carried into apical part in order to protect the cells from acid damage • Fenestrated capillaries also facilitate delivery of HCO3- • In antrum where HCO3- secreting parietal cells are few blood supply is increased in order to facilitate removal of acid
Gastric nerves • Parasympathetic sympathetic [ vagus] Anterior br Posterior br (frm rt vagus) ( frm Lt vagus)
Gastric Anterior nerve Pyloric Gastric nerve radiates on anterior surface of body &fundus One br which is larger near lesser curvature is called greater anterior gastric N (anterior nerve of latarjet)
2 in no: one which traverses the lesser omentum almost horizontally to Rt, then turns down on the left side of hepatic artery to reach pylorus Other arises from greater anterior gastric nerve & passes obliqly to pylorus Pyloric br
Posterior Gastric coeliac Gastric Radiate over the posterior surface of body & fundus upto pyloric antrum Largest pass along lesser curvature Greater posterior gastric nerve Coeliac Pass to coelic plexus
Sympathetic supply • From Coeliac plexus Hepatic plexus Lt phrenic plexus Inconstant brs Lt thorasic nerve, thorasic & lumbar trunks • Form Sub mucosal plexus of Meissner Myentric plexus of Auerbach
Arranged in 4 groups 1st gp accompany Lt gastric artery. Receives a large area on both gastric surface. They end in Lt gastric nodes 2nd gp short gastric & Lt gastro epiploic arteries. Drains Left of the vertical from oesophagus. End in pancreaticosplenicnode Lymphatics are continous with that of oesophagus & duodenum
3rd gp drains Rt half of grtr curvature as far as pylorus. End in Rt gastro epiploic nodes which drain to pyloric nodes 4th gp Pylorus Drains to hepatic, pyloric & Lt gastric nodes
Although these vessels communicate, their valves direct lymph from Rt part of stomach towards lesser curvature. From Lt side to greater curvature
PHYSIOLOGY • Parietal cellsHCL & IF • Chief cells pepsinogen • ECL histamine
Gastric secretions • 2500 ml/day • Contents • cations Na,K,Mg,H+ anions Cl,HPO2,so4 pepsin lipase Mucus IF
MUCOSAL BARRIER • Formed by mucous & HCO3- • Mucous made of glycoprotein forms a flexible gel coat • They also protect duodenal mucosa • Their stimulation is augmented by prostaglandin • Trefoid peptides also provide protection