Download
1 / 45
450 likes | 615 Views
Pediatric pharyngeal diseases. Ehab ZAYYAN, MD, PhD Hacettepe University- Turkey Consultant and Head of ENT Department European Gaza Hospital Assist. Professor, School of Medicine Islamic University, Ga za. Anatomy of the pharynx. The pharynx.

E N D
Pediatric pharyngeal diseases Ehab ZAYYAN, MD, PhD Hacettepe University- Turkey Consultant and Head of ENT Department European Gaza Hospital Assist. Professor, School of Medicine Islamic University, Gaza
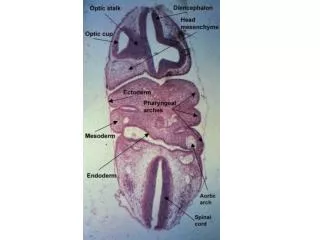
The pharynx • The pharynx is located behind the nasal cavities, the mouth and the larynx • From the skull base till the C6 • It is a musculu- membranous wall that is deficient anteriorly.
The lateral and posterior walls of the pharynx consist of 3 pairs of muscles which unite in the posterior midline at the pharyngeal raphe. • Superior constrictor muscle • Middle constrictor m • Inferior constrictor muscle.
Nasopharynx • It lies behind the nasal cavities, above the soft palate. • The pharyngeal tonsil (adenoid): a collection of lymphoid tissue in the submucosa of this region
The Eustachian tube orifice opens into the lateral wall of the nasopharynx • Tubal tonsils: a collection of lymphoid tissue in the submucosa behind the opening of the auditory tube
Oropharynx • From the soft palate to the upper border of the epiglottis • Roof: undersurface of the soft palate • Floor: root of the tongue • Anterior wall: oropharyngeal isthmus • Posterior wall: C2, C3
Oropharynx lateral wall • Palatoglossal fold • Palatopharyngeal fold • Uvula • Palatinal tonsils
Palatine tonsils • Two masses of lymphoid tissue located in the tonsillar fossa. • The tonsil is covered by mucous membrane and its medial surface is free projecting in the cavity of the pharynx • Tonsillar crypts on the surface. • Fibrous capsule covers the lateral surface of the tonsil. It separates it from the superior constrictor pharyngeal muscle.
Waldeyere’s ring of lymphoid tissue At the junction of the mouth and oropharynx and the nose with the nasopharynx there is a collection of lymphoid tissue: • Palatine tonsils • Lingual tonsils • Pharyngeal tonsils • Tubal tonsils
Hypopharynx (laryngopharynx) • From the upper border of the epiglottis till the lower border of the cricoid cartilage.
Lymph drainage of the pharynx • Nasopharynx→ retropharyngeal nodes • Tonsils and oropharynx → upper deep cervical nodes, especially the jugulodigastric node which is called the tonsillar node. • Hypopharynx → vessels thru the thyrohyoid membrane → upper deep cervical nodes
Acute pharyngitis • Mostly a viral infection • Fever, sore throat, odynophagia, malasia • Recovery within 5 – 7 days • Tx: analgesics ….
Acute tonsillitis • Very common in pediatric population • Fever, sore throat, malasia, dysphagia, neck swelling….. Etiology: • Viruses: IMN, herpes… • Group A, B-hemolytic streptococci • Diphteria
Acute tonsillitis Diagnosis • Physical examination is the most important • Red swollen tonsils, follicular, membranous… • Cervical lymphadenopathy • CBC • ASOT • Cultures
Acute tonsillitis Treatment • Penicillin: Penicillin G Procaine penicillin Benzathine penicillin • Single dose benzathine penicillin is the best choice • < 30 kg child: 600.000 IU im • >30 kg child: 1200.000 IU im
Acute tonsillitis Oral antibiotics (10 days of tx) • Penicillin V (oral suspension) • Amoxicillin • Erythromycin • 2nd line….. Analgesia, fluids and bed rest are very important
Scarlet fever • Scarlet fever is secondary to acute streptococcal tonsillitis or pharyngitis with production of endotoxins by the bacteria. • Manifestations include an erythematous rash, severe lymphadenopathy with a sore throat, vomiting, headache, fever, erythematous tonsils and pharynx, tachycardia, and a yellow exudate over the tonsils, pharynx, and nasopharynx. • A strawberry tongue with a rash and large glossal papillae is a good diagnostic sign
Poststreptococcal glomerulonephritis • The typical patient develops an acute nephritic syndrome 1 to 2 weeks after a streptococcal infection. • The infection is secondary to the presence of a common antigen of the glomerulus with the streptococcus. • Penicillin management may not decrease the attack rate, and there is no evidence that antibiotic therapy affects the natural history of glomerulonephritis. • A tonsillectomy may be necessary to eliminate the source of infection.
Acute rheumatic fever • Mostly 5 – 15 years of age • Occurs at the 3rd to 9th day of infection • Johns criteria : major and minor • Penicillin prophylaxis • Tonsillectomy
Peritonsillar abscess • The spread of infection is from the tonsil with pus formation between the tonsil bed and the tonsillar capsule • Fever, severe throat pain, dysphagia, odynophagia, trismus, drooling… • It may lead to airway obstruction, aspiration or parapharyngeal and retropharyngeal abscess formation • Treatment: incision and drainage, iv AB, tonsillectomy
Parapharyngeal space abscess • Parapharyngeal space: between the lateral pharyngeal wall and the mandible • Contains dangerous structures like the carotid artery and the jugular veins. • Tonsillitis, dental infections, sinusitis, lymphadenitis….can lead to parapharyngeal cellulitis or abscess • Dx: clinical, USG, CT • Tx: iv AB + incision and drainage (lateral cervical approach)
Retropharyngeal space infections • Mostly in children < 2 years • Retropharyngeal space: between the pharynx and the prevertebral fascia, extending from the skull base into the mediastinum till tracheal bifurcation • irritability, fever, dysphagia, muffled speech, noisy breathing, stiff neck, and cervical lymphadenopathy. • Posterior pharyngeal wall bulging • Cellulitis vs abscess • Tx: transoral/ external incision
Chronic tonsillitis • Recurrent acute tonsillitis • Chronic tonsillar and pharyngeal inflammation: pain, irritation, smagma, halitosis, tonsilolithiasis… • Hypertrophic tonsils
1.Infection Recurrent, acute tonsillitis (more than six episodes per year or three episodes per year for 2 years) Chronic tonsillitis: halitosis, persistent sore throat, tender cervical adenitis Peritonsillar abscess 2. Obstruction Excessive snoring and chronic mouth-breathing Obstructive sleep apnea or sleep disturbances 3. Neoplasia Asymmetric tonsillar hypartrophy Indications for tonsillectomy
Adenoid diseases • Common in young children • Adenoid hypertrophy caused by: infections, allergy, environmental.. • Symptoms • Otitis media and sinusitis • Dx: palpation, X-ray, endoscopy • Tx: Surgery
Indications for adenoidectomy • Recurrent purulent adenoiditits • Adenoid hypertrophy associated with otitis media • Adenoid hypertrophy associated with chronic sinusitis • Adenoid hypertrophy associated with excessive snoring and chronic mouth-breathing • Sleep apnea or sleep disturbances • Speech abnormalities • Neoplasia suspesion
Contraindications of adenotonsillectomy • Bleeding abnormalities • Acute infections • Cleft palate?? • Age???