Download
1 / 39
390 likes | 579 Views
Comments on JNC 7: including N.O.D.*. Ray Townsend, MD #4 on NHLBI most-wanted list September 28, 2005. 48 year old T2DM man. Feels OK Diabetes is under good control Takes only one med (for DM) BMI is 30.6 kg/m 2 “I’m working on it” (BMI was 31.3 a year ago)

E N D
Comments on JNC 7: including N.O.D.* Ray Townsend, MD #4 on NHLBI most-wanted list September 28, 2005
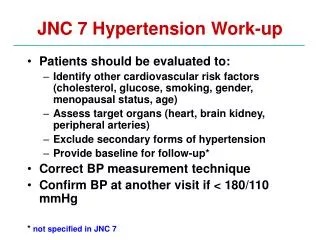
48 year old T2DM man • Feels OK • Diabetes is under good control • Takes only one med (for DM) • BMI is 30.6 kg/m2 • “I’m working on it” (BMI was 31.3 a year ago) • Blood pressure is 134/82 mm Hg • Does he have “hypertension”?
Classification and Management of BP for adults *Treatment determined by highest BP category. †Initial combined therapy should be used cautiously in those at risk for orthostatic hypotension. ‡Treat patients with chronic kidney disease or diabetes to BP goal of <130/80 mmHg. JNC 7 slideset
CON #1 • Definition of “hypertension” amongst those with a “compelling indication” is confusing
Surveillance visit Feels well Bp 134/78 mm Hg Heart rate 64 bp Exam pretty unremarkable Insurer asked for EST – done (and normal) Meds: 2 anti-diabetic meds atorvastatin 100 mg losartan 25 mg HCTZ 25 mg spironolactone 10 mg amlodipine 100 mg metoprolol XL 60 year old diabetic woman
Hypertension is ... “the level of blood pressure at which the benefits of action (i.e. therapeutic intervention) exceed those of inaction.” • Evans and Rose Brit Med Bull 1971;27:37-42
CON #2 • It’s not clear when you stop adding or titrating: when does drug toxicity (and cost) equal or outweigh benefit?
JNC 7 on metabolic syndrome • No special consideration in drug treatment of this entity – reference is only to the generic treatment algorithm • The peculiarities of the diagnostic criteria of this condition contain several metabolic aspects where a diuretic (the preferred agent) is probably not the best choice
CON #3 • More evidence needed in (particulars of) drug treatment of metabolic syndrome, particularly in light of ACE/ARB ‘benefits’ on development of type 2 diabetes during treatment
Risk adverse • What is the point in treating hypertension? • To reduce the RISK of target organ damage • How is CV risk factored into JNC 7 treatment recommendations?
To be fair • The compelling indications do much to identify patients with enhanced risk • Diabetes, proteinuria/CKD, MI etc.
CON #4 • More is needed in terms of risk management and choice of agent(s) and non-hypertensive medications
Hypertension for many years; not well managed for the first 5 years; “better” now Positive family history of CKD/dialysis Not diabetic, +1 proteinuria BP is 136/76 mm Hg ACE Loop DHP-CCB Beta-blocker 49 year old AA with an eGFR = 48
JNC 7 recommendation Hypertension 2003;42:1225
The evidence BP in USUAL group 141/85 mm Hg BP in LOWER group 128/78 mm Hg JAMA 2002;288:2421-2431
CON #5 • The data on GFR preservation, in the absence of significant proteinuria, are wanting (but there are other target organs at risk)
Average response to guidelines? JNC 7 ATP III Guidelines 4 dummies
Report (JAMA, 1977) 1980 Report (Archives) 1984 Report (Archives) 1988 Report (Archives) JNC V (Archives, ‘93) JNC VI (Archives ‘97) JNC 7 (Hypertension ‘03) 6 pages 6 pages 13 pages 16 pages 30 pages 34 pages 47 pages History
CON #6 • The Report is pretty thorough, but can we do better in terms of reader ‘friendliness’?
JNC 7 & ALL HAT (NHLBI)? ALL HAT
But what about? • The metabolic consequences of diuretic use? • More diabetes* • More hypokalemia • (higher) cholesterol and triglyceride • Higher uric acid levels
From the ALL HAT report • Among individuals classified as non-diabetic … the incidence of new-onset diabetes was 11.6% (chlorthalidone) 9.8 % (amlodipine) and 8.1 % (lisinopril) • “Overall these metabolic differences did not translate into more cardiovascular events … or mortality…” JAMA 2002;288:2989
PIUMA study • observational registry of M & M • initially untreated essential hypertension subjects • initiated June 1986 • hypertension by standard definitions • EKG used Cornell voltage • 24 hour ABPM done • diabetes = glucose > 7 mmol/L (126 mg/dl) • n=875 subjects
PIUMA study (Verdecchia) Hypertension 2004;43:963-970
chronic heart failure left ventricular hypertrophy U.S. residency Hispanic ethnicity black race previous stroke increased body mass index low serum high-density lipoprotein high non-fasting serum glucose elevated systolic blood pressure increased age female gender and history of antihypertensive drug use Narayan JAMA 2003 Cooper-DeHoff Circ 2003 Lindholm J Hypertens 2002 What factors predict N.O.D. ??
Which factor should I focus on? • Pretreatment glucose
CON #7 • New onset diabetes may not be as benign as indicated by the short follow up in ALL HAT • However, sight should not be lost of blood pressure control (which generally trumps blood sugar control in RCTs)
For further contact etc .… • Positive comments • townsend@mail.med.upen.edu • Criticisms? • Dial 1-800-hows my lecture • Or email Dr Moser