Download

1 / 55
550 likes | 1.12k Views
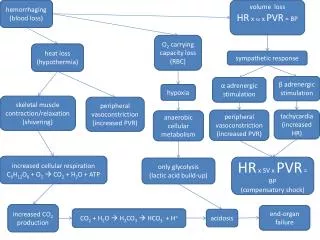
BLOOD LOSS. COLLATERALS IN VERTEBRAL VENOUS PLEXUS. GASTRIC INFLATION, COUGHING, BUCKING, ↑ Paw. SANDBAGS MATTRESSES. PRESSURE ON IVC. BLOOD LOSS. COLLATERALS IN VERTEBRAL VENOUS PLEXUS. ↑↑ BLEEDING. PRESSURE ON IVC. BLOOD LOSS. ANESTHETIC FACTORS. SURGICAL FACTORS:. POSTURAL FACTORS.

E N D
BLOOD LOSS COLLATERALS IN VERTEBRAL VENOUS PLEXUS GASTRIC INFLATION, COUGHING, BUCKING, ↑Paw SANDBAGS MATTRESSES PRESSURE ON IVC
BLOOD LOSS COLLATERALS IN VERTEBRAL VENOUS PLEXUS ↑↑ BLEEDING PRESSURE ON IVC
BLOOD LOSS ANESTHETIC FACTORS SURGICAL FACTORS: POSTURAL FACTORS BLOOD LOSS RESPIRATORY FACTORS
BLOOD LOSS SURGICAL FACTORS: • EXTENT OF DISSECTION • DURATION OF SUGERY • SITE AND SIZE OF BONE GRAFT • PREVIOUS SPINAL FUSION • SURGICAL TECHNIQUE • 15-25 mL/kg in uncomplicated spine fusion • with Harrington rods or cotrel-dubousset instrumentation • Massive blood loss: • Anterior posterior spine fusion • Instrumentation into pelvis • Osteotomy of spine to correct rigid abnormalities
BLOOD LOSS ANESTHETIC FACTORS INCREASED ARTERIAL PRESSURE INCREASED PRESSURE ON VERTBRAL VENOUS PLEXUS
BLOOD LOSS POSTURAL FACTORS INCREASED ABDOMINAL WALL TENSION INCREASED INTRA- ABDOMINAL PRESSURE EXTRINSIC PRESSURE
BLOOD LOSS INTERMITTENT POSITIVE PRESSURE VENTILATION INCREASED PRESSURE ON IVC DIVERSION TO VERTEBRAL VENOUS PLEXUS RESPIRATORY FACTORS
BLOOD LOSS: • Calculate MABL • Judicious blood transfusion • Consider alternatives: • Autologous tranfusion • Induced hypotension • Pre-operative Autologous Blood Donation • Normovolemic or hypervolemic hemodilution • Cell salvage
MINIMISING BLOOD LOSS • SURGICAL TECHNIQUE: Sub-periosteal dissection Compressing wound edge with finger tips Packs and retractors • MINIMISE INTRA- ABDOMINAL PRESSURE- (vertebral venous plexus bleeding) Special frames – Relton –Hall frame Adequate muscle relaxation Deep plane of anesthesia Abdomen free of pressure
MINIMISING BLOOD LOSS 3. INFILTRATION WITH EPINEPHRINE: Local vasoconstriction & hydrostatic pressure of fluid volume Maximum dosage with volatile anesthetics- Halothane – 1.0 μg/kg Isoflurane – 3.5 μg/kg (sevo/ des) Enflurane – 5.5 μg/kg Arrhythmias – rare in children
MINIMISING BLOOD LOSS • 5. DELIBERATE HYPOTENSION: • Decreases blood loss by 30-50% when MAP is maintained between 50-60 mmHg. • Concern: Deliberate hypotension reduces SCBF during distraction of spine. • Returns to normal in 35 min. • Hence, distraction no more than 35 min after the start of delberate hypotension. • morbidity of 0.85 per cent • Mortality- between one in 200 and one in 500 patients • Disadvantage- if cardiac arrest or accidental extubation occurs, the patient is in an inappropriate position for therapy
Slowly over 10-15 min • Cerebral, coronary, renal vasodilation • SBP – 75 mmHg • Warning signs: • Excessively dry field • Dark venous blood • Deterioration of SSEPs • Arterial cannulation • U. output – 0.5 mL/kg/hr
Near- normal PaCO2 and SCBF. • PETCO2- reliable estimate of paCO2 in children • Adults – Vd/Vt increases
BLOOD LOSS • 2. Hemodilution – • Upto a hematocrit of 20-25% • Withdraw blood (if isovolemic) • Replace with 3 units crystalloids or 1 unit colloid for every 350 -400 ml of blood withdrawn • Intraop. Assessment of Hb and H‘crit. • Jehovah’s witness
Blood loss 2. PRE-OPERATIVE AUTOLOGOUS BLOOD DONATION: • Replace blood loss with autologous blood • Prevents complications of allogenic blood • IDEAL PATIENT: • Healthy to undergo elective surgery • Likely to need transfusion after surgery • Has Hb > 11g/dL
BLOOD LOSS… • AMERICAN ASSOCIATION OF BLOOD BANKS: • No less than 4 days between donations • No less than 3 days before surgery • Once a week donations for three weeks prior to surgery. • Complications: • Lightheadedness • Vasovagal reaction • Delay surgery • Cost • Inconvenience • Not applicable to Jehovah’s witness
CONTRAINDICATIONS: • Bacteremia • Decreased oxygen delivery( fixed output, anemia, hypoxemia) • Pediatric age group • ?HUMAN ERYTHROPEITIN OR IRON ADJUNCTS • Erythropoeitin: • 600 U/kg twice weekly • 400 U/kg s.c. once a week for 4 weeks (Kulier)
BLOOD LOSS • 3. Cell- salvage: • 50-60% of RBCs can be salvaged • Recover- concentrate- wash- return to patient • Disadvantage- lack of plasma and platelets • INDICATIONS: • Children > 10kg • Blood loss – 20% of blood volume • Procedures in which more than 10% pts are tranfused more than 1 unit blood
CELL SALVAGE ANTICOAGULANT TRANSFUSION (Hcrit- 50 -70%) SALINE WASTE PRODUCTS (WBCs,anticoag, contaminants) STERILE RESERVOIR CENTRIFUGE (5000 rpm)
PROCESSED BLOOD: • Thrombocytopenia • Hypofibrinogenemia • Platelet dysfunction • DIC
CONTRAINDICATIONS: • Extravasated blood > 6 hrs • Excessively hemolysed blood • Bowel contents • Malignant cells • Microfibrillar collagen hemostat • ?Sickle cell anemia • ? Jehovah’s witness
BLOOD LOSS… • 4. Anti-fibrinolytic agents: • Tranexamic acid and EACA: • Hypotension • Cautious during induced hypotension • Better in paediatric patients and neuromuscular disease • DDAVP: • Increases Vwf. • Single dose og 10 mcg/sq.m – dec 30 % loss • Worsen SIADH
AIR EMBOLISM • AIR EMBOLISM: • High risk- 50% • CVC in place • Detection- ETCO2, Bubbling in the wound (1st sign) • Transthoracic doppler ECHO • TEE • Treat- Flood field with saline • Switch of N2O • IV fliuids
EVOKED POTENTIALS SOMATO SENSORY EVOKED POTENTIALS
EVOKED POTENTIALS • SSEPs: • Stimulus: Peripheral nerve • Pathway: Posterior column • Cerebral cortex • EEG scalp electrodes
SSEPs…. • Latency • Amplitude • Increase in latency or decrease in amplitude is taken as surgical injury or ischemia unless proved otherwise • Latency – inc by 10-15% • Amplitude – dec by 50% - CAUSE FOR CONCERN
SSEP… Amplitude Latency
Motor EVOKED POTENTIALS MOTOR EVOKED POTENTIALS
MEPs • MEPs: • Stimulus: Motor cortex • Pathway:Anterior column • Motor nerve- electromyographic signals, peripheral electrodes, actual limb movements • EEG scalp electrodes
ANESTHETIC REGIMEN • Avoid pre-medication • Induction – short acting drugs, short acting relaxants • Supplemental opioid boluses • Maintenance- 50% N2O + volatile anesthetic 0.25 MAC • Or infusion of etomidate 0.01-0.02 mg/kg/min or propofol 0.1-0.2 mg/kg/min • Discontinue 30 -45 min before testing and continue with etomidate or ketamine infusion at low doses. • Keep TOF at 3-4 • NTG or esmolol infusion – hemodynamic stability
WAKE UP TEST • PRINCIPLE: “Lighten” the anesthetic plane sufficiently to allow the patient follow commands • WHEN TO PERFORM? • Distraction of spinal column • After all instrumentation is in place • PROCEDURE: • Pre- op counselling and rehearsal • Prepare adequate narcotic and i.v. induction agent
Monitor muscle relaxation- allow adequate spontaneous respiration or TOF count of 4 • Reduce inhalational agent to MAC 0.5 • R/O resp. depression by narcotic (?Naloxone) • Command patient to squeeze your hand • Move leg
COMPLICATIONS: • Extubation in prone position • Recall • MI • Self injury • Dislodgement of instrumentation • Air embolism from open venous sinuses
EXTUBATION • INDIVIDUALISED DECISION: • Pre-operative decision • Adult idiopathic scoliosis with mild to moderate PFT abnormailties- EXTUBATION IN OR • PRE- OPERATIVE FACTORS: • Severe PFT derangement- (VC<30% predicted), Abnormal blood gases- MECHANICAL VENTILATION • INTRA OPERATIVE FACTORS: • Pleural nick by surgeon • Antero- lateral or anterior approach • Thoracotomy or lung collapse • Abnormal blood gases
PRE- EXTUBATION FACTORS: • VC> 10mL /kg • TV>3mL/kg • RR spont < 30/min • NIF >-30 cmH2O
POST OPERATIVE CARE • Chest physiotherapy: • Coughing • Deep breathing • Incentive spirometry • Bronchodilators • Pain relief • Multimodal • Systemic- continuos / intermittent/ PCA • Epidural- intermittent/ continous/ PCEA
RESPIRATORY FUNCTION AFTER SCOLIOSIS CORRECTION • Lung volumes – reduced for 1st 10 days • PaO2 – recuced for 2 days • PaCO2 and pH – normal • FRC – normalises on 5th post operative day • Mechanical properties of chest wall • Pain – reduced expansion • Rib configuration • Chest wall edema • Impaired resp. muscle function
Mechanical properties of lungs: • Increased lung water • Increased surface tension • Atelectasis • Inability to cough • Infection
LONG TERM CHANGES • Lung volume – unaltered • Gas – exchange – improved • Dead space – reduced by 40% • Hypoxemia – relieved • Ventilatory equivalent – reduced by 20% • Regional blood flow – improved
CONCERNS: • Pre-incisional infiltration • Sub-periosteal resection • Stripping of erector spinae- • Osteotomy and wedge resection of vertebre • Distraction • Instrumentation
Other approaches • ANTERIOR APPROACH: • Presence of co-existing vertebral anomaly (spina- bifida or hemi- vertebrae) CONCERNS: Blood loss – lesser than posterior approach Full muscle relaxation High FiO2 and selective one-lung ventilation Post-operative hypoventilation Atelectasis Pain Infection
COMBINED APPROACH: • Anterior and posterior • Single or multiple stages • Massive blood loss and repeated positioning
LASER SPINE SURGERIES • CO2 laser • Holmium, Nd YAG lasers • Minimal blood loss • Acceptable correction with minimal scarring • Disadvantages: • Expertise • Economic constraints • Laser hazards