Download
1 / 27
270 likes | 287 Views
Psychological Therapies for Risk Reduction. Dr Barbara Hedge Consultant Clinical Psychologist. Is there more to risk prevention than MI?. Flavour of the month Relaxation therapy Cognitive behaviour therapy Solution focused therapy Motivational interviewing Why recommended

E N D
Psychological Therapies for Risk Reduction Dr Barbara Hedge Consultant Clinical Psychologist
Is there more to risk prevention than MI? • Flavour of the month • Relaxation therapy • Cognitive behaviour therapy • Solution focused therapy • Motivational interviewing • Why recommended • Looks to be effective but cheap • Never mind the problem
Putting therapy into context • Sexual health setting • A normal, universally practised behaviour • Risk • Probability of danger and/or undesired outcomes • Individual • Partners and families • Society • Undesired outcomes • Sexually transmitted infections • Pregnancy • Aim to change behaviours to reduce risk • Identify useful psychological therapies
What factors are associated with risk? • Lack of knowledge or understanding • Resources • Skills • Communication • Ability • Conceptualisation of personal risk • Motivation to reduce risk • Lack of care for self or others • Low mood • Shame • Power differential • Cultural • Coercive
Sexual health expert knows best • Assumptions • Patients are always rational so act on knowledge • The goals of patients are the same as goals of sexual health practitioners • All patients want what is best for themselves • UK national guidelines on safer sex advice • BASHH 2011 • Conclusions • Giving knowledge is all that is necessary • Telling people what to do is the same as giving advice
They just don’t listen! • Repeated STIs • HIV transmission • Unwanted pregnancies • Repeated requests for PEP Information is necessary but not sufficient
Conceptualisation of personal risk andmotivation to reduce risk
Theory of reasoned action • Fishbein, 1979
Which therapy? • What, who needs to change? • Who wants or doesn’t want to change? • What are the risk factors • Goal to be achieved • How to bring about change • Learning theories • Skinner’s Operant Conditioning theory • Bandura’s Social Learning theory
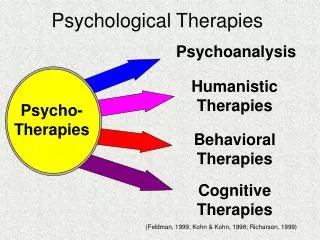
Behaviour change therapies • Cognitive Behaviour Therapy • Systemic Therapy • Solution focussed Therapy • Motivational Interviewing • Peer Influence • Nudge
Personal risk cognitions • Not want to transmit • Not want to disclose • Not want to use a condom • Not want to become infected • Not want to think about it • Not want to confront
Self-serving attributions • Constructed narratives that allow justification of our behaviours • Before and/or after action or non-action • ART means I have no virus to transmit • PEP is available if need it • If partner is willing to have unprotected sex they are probably already positive • Partner wouldn’t suggest unprotected sex if they were positive • Can trust negotiated safety agreement
Cognitive behaviour therapy • Addresses non-adaptive cognitions • Replaces with adaptive • Can confront the issue • Can plan to remain uninfected • Raises mood • Lowers anxiety • Increases self-esteem • Adoption of self affirming behaviours • Assertiveness • Acceptance of rejection of the behaviour rather than of the self
Learning new behaviours • Operant Conditioning • Reinforcement • Positive repeat of behaviour • Great sex with a condom • Remove negative • Finally agree to sex when agree to condom • Negative • Fail to keep erection with a condom • Remove positive • No sex as no condoms
Nudge theory • Suggestion + positive reinforcement • Address one element of behaviour in the chain • If positively reinforced by others or internally • Repeat behaviour • Reinforce additional elements in chain • Gradually approach goal of protected sex
Solution focussed therapy • Not concentrating on the problem • Uses resources patient already has • Encourages trying a course of action (possible solution) • Strengths patient already has • Advantages • Quick • Cheap • Patient generated • Builds self esteem and self efficacy • Disadvantages • Failure for complex issues • Key factors may not be identified • Difficult engagement when depressed
Motivational interviewing • Directive, client-centredcounselling style to resolve ambivalence (Rollnick & Miller, 1995) • Motivation = Importance + Confidence + Readiness • Aims to elicit and boost these factors • NICE • Quick • Cheap • Catch people on first visit • Evidence of effectiveness • A stand alone intervention • Possible service approach
Peer interventions • Use of a peer educator • Group leader • Introduce safer sex into conversation • Set up group norm • ‘cool to use condoms’ • Social learning theory + Nudge + MI • Efficacy • Some support • ? Culturally specific • Review: Simoni et al, AIDS Behav, 2011, 1589-95
When do I need systemic therapy? • Risky sex is rarely an individual practice • What is the influence of the partner? • What is the perceived influence of the partner • Is there a power in-balance? • Communication • Negotiation • Agreement between partners to change
Summary • Motivational interviewing a good place to start • Finding out the whole picture • Patient suggests the next step • Moves to action from pre-contemplation • More commitment to meet their own challenge • Ready to address cognitions and beliefs and learn skills • Able to identify when there are greater unmet needs • Pathways for onward referral to meet general needs • Appropriate use of therapeutic techniques brings best results