Download
1 / 1
10 likes | 128 Views
Investigation. Characteristic. Frequency in no. and %. Ultrasound finding. Size. <5 cm 5-10 cm >1T0 cm. 11 (12.6%) 54 (62.1%) 22 (25.3%). Total. 87 (100%). Location. Unilateral Bilateral. 83 (97.6%) 2 (2.4%). Total. 85 (100%). Side.

E N D
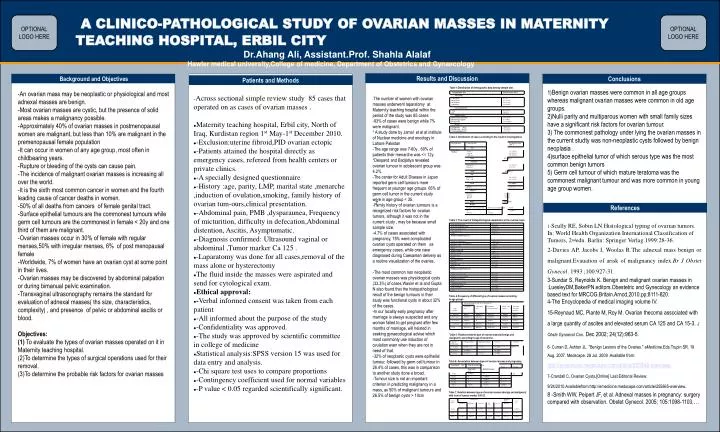
Investigation Characteristic Frequency in no. and % Ultrasound finding Size <5 cm 5-10 cm >1T0 cm 11 (12.6%) 54 (62.1%) 22 (25.3%) Total 87 (100%) Location Unilateral Bilateral 83 (97.6%) 2 (2.4%) Total 85 (100%) Side Right side Left side 59 (67.8%) 28 (32.2%) Total 87 (100%) Ascitis 2 (2.3%) Report Negative Normal Raised 51 (69%) 15 (20%) 8 (11%) Total 74 (99.9%) Report Negative for atypical cells Positive for atypical cells Total 36 (94.7%) 2 (5.3%) 3(100%) Gestational age Type of ovarian masses Total P value Functional cyst Epithelial tumor 5 wks 1(100%) 0 1 0.2 12 wks 0 1(100%) 1 17 wks 0 *1(100%) 1 38 wks 0 1(100%) 1 Total 1(25%) 3(75%) 4(100%) A CLINICO-PATHOLOGICAL STUDY OF OVARIAN MASSES IN MATERNITY TEACHING HOSPITAL, ERBIL CITY Dr.Ahang Ali, Assistant.Prof. Shahla Alalaf Hawler medical university,College of medicine, Department of Obstetrics and Gynaecology OPTIONALLOGO HERE OPTIONALLOGO HERE Results and Discussion Background and Objectives Conclusions Patients and Methods 1)Benign ovarian masses were common in all age groups whereas malignant ovarian masses were common in old age groups. 2)Nulli parity and multiparous women with small family sizes have a significant risk factors for ovarian tumour. 3) The commonest pathology under lying the ovarian masses in the current studty was non-neoplastic cysts followed by benign neoplasia . 4)surface epithelial tumor of which serous type was the most common benign tumors 5) Germ cell tumour of which mature teratoma was the commonest malignant tumour and was more common in young age group women. Table 1:Distribution of demographic data among sample size. -An ovarian mass may be neoplastic or physiological and most adnexal masses are benign. -Most ovarian masses are cystic, but the presence of solid areas makes a malignancy possible. -Approximately 40% of ovarian masses in postmenopausal women are malignant, but less than 10% are malignant in the premenopausal female population -It can occur in women of any age group, most often in childbearing years. -Rupture or bleeding of the cysts can cause pain. -The incidence of malignant ovarian masses is increasing all over the world. -It is the sixth most common cancer in women and the fourth leading cause of cancer deaths in women. -50% of all deaths from cancers of female genital tract. -Surface epithelial tumours are the commonest tumours while germ cell tumours are the commonest in female < 20y and one third of them are malignant. -Ovarian masses occur in 30% of female with regular menses,50% with irregular menses, 6% of post menopausal female -Worldwide, 7% of women have an ovarian cyst at some point in their lives. -Ovarian masses may be discovered by abdominal palpation or during bimanual pelvic examination. -Transvaginal ultrasonography remains the standard for evaluation of adnexal masses( ths size, characteristics, complexity) , and presence of pelvic or abdominal ascitis or blood. Objectives: (1) To evaluate the types of ovarian masses operated on it in Maternity teaching hospital. (2)To determine the types of surgical operations used for their removal. (3)To determine the probable risk factors for ovarian masses -Across sectional simple review study 85 cases that operated on as cases of ovarian masses . • Maternity teaching hospital, Erbil city, North of Iraq, Kurdistan region 1st May-1st December 2010. • -Exclusion:uterine fibroid,PID ovarian ectopic • -Patients attained the hospital directly as emergency cases, refereed from health centers or private clinics. • -A specially designed questionnaire • -History :age, parity, LMP, marital state ,menarche ,induction of ovulation,smoking, family history of ovarian tum-ours,clinical presentation. • -Abdominal pain, PMB ,dysparaunea, Frequency of micturition, difficulty in defecation,Abdominal distention, Ascitis, Asymptomatic. • -Diagnosis confirmed: Ultrasound vaginal or abdominal ,Tumor marker Ca 125 . • -Laparatomy was done for all cases,removal of the mass alone or hysterectomy • The fluid inside the masses were aspirated and send for cytological exam. • Ethical approval: • -Verbal informed consent was taken from each patient • -All informed about the purpose of the study • -Confidentiality was approved. • -The study was approved by scientific committee in college of medicine • Statistical analysis:SPSS version 15 was used for data entry and analysis. • -Chi square test uses to compare proportions • -Contingency coefficient used for normal variables • -P value < 0.05 regarded scientifically significant. -The number of women with ovarian masses underwent laparatomy at Maternity teaching hospital within the period of the study was 85 cases -93% of cases were benign while 7% were malignant. * A study done by Jamal et al at institute of Nuclear medicine and oncology in Lahore Pakistan -The age range was 7-60y , 60% of patients their menarche was <= 12y. *Despand and Badjatiya revealed ovarian tumour in adolescent group was 4.2% . -The center for Adult Disease in Japan reported germ cell tumours more frequent at younger age groups. 65% of germ cell tumor in the current study were in age group < 35. -Family history of ovarian tumours is a recognized risk factors for ovarian tumors, although it was not in the current study , may be because small sample size. -4.7% of cases associated with pregnancy, 75% were complicated ovarian cysts operated on them as emergency cases, while one case diagnosed during Caesarean delivery as a routine visualization of the ovaries. -The most common non neoplastic ovarian masses was physiological cysts (33.3%) of cases,Wasim et al and Gupta N also found that the histopathological result of the benign tumours in their study was functional cysts in about 32% of the cases. -In our locality early pregnancy after marriage is always suspected and any woman failed to get pregnant after few months of marriage, will heisted in seeking gynaecological advise which most commonly use induction of ovulation even when they are not in need of that. -32% of neoplastic cysts were epithelial tumour, followed by germ cell tumour in 26.4% of cases, this was in comparison to another study done a broad. -Tumour size is not an important criterion in predicting malignancy in a mass, as 50% of malignant tumours and 26.5% of benign cysts > 10cm Table 2: Distribution of cases according to the result of investigations 7 References Table 3: The result of histopathological examination in the ovarian mass. 1-Scully RE, Sobin LN.Histological typing of ovarian tumors. In: World Health Organization International Classification of Tumors, 2ndedn. Barlin: Springer Verlag.1999:28-36. 2-Davies AP, Jacobs I, Woolas R.The adnexal mass benign or malignant.Evauation of arisk of malignancy index.Br J Obstet Gynecol. 1993 ;100:927-31. 3-Sundar S, Reynolds K. Benign and malignant ovarian masses in :LuesleyDM,BakerPN.editors.Obestetric and Gynecology an evidence based text for MRCOG.Britain.Arnod,2010.pp;8111-820. 4-The Encyclopedia of medical imaging volume IV. 15-Reynaud MC, Plante M, Roy M. Ovarian thecoma associated with a large quantity of ascites and elevated serum CA 125 and CA 15-3. J Obste Gynaecol Can. Dec 2002; 24(12):963-5. 6- Curran D, Ashton JL. "Benign Lesions of the Ovaries." eMedicine.Eds.Trupin SR. 19 Aug. 2007. Medscape. 28 Jul. 2009 .Available from: http://emedicine.medscape.com/article/265548-overview. 7-Crandall C. Ovarian Cysts.[Online] Last Editorial Review: 9/24/2010.Availablefrom:http://emedicine.medscape.com/article/255865-overview. 8 -Smith WW, Peipert JF, et al. Adnexal masses in pregnancy: surgery compared with observation. Obstet Gynecol. 2005; 105:1098-1103.… Table- 4:Frequency of different type of ovarian masses according to age groups Table 5: Relation between type of ovarian masses (benign and malignant) according to age of menarche. Table 6: Association between types of ovarian masses and pregnancy. Table 7: Relation between types of ovarian masses (benign and malignant) with level of tumour marker CA125.