Download
1 / 57
570 likes | 678 Views
Applying Decision Science and Game Theory to Suicidal Behaviors Decision-Making Models of Functional Psychopathology. Lawrence Amsel, MD, MPH Director of Dissemination Research for Trauma Studies and Services Collaborators / Co-authors Avital Pilpel Randall Marshall.

E N D
Applying Decision Science and Game Theory to Suicidal BehaviorsDecision-Making Models of Functional Psychopathology
Lawrence Amsel, MD, MPH Director of Dissemination Research for Trauma Studies and Services Collaborators / Co-authorsAvital Pilpel Randall Marshall
Applying Decision Science to Clinical Psychiatry • Examples of application of models and concepts from decision science to clinical psychiatry • Modeling Ambivalent Suicide Attempts • Effecting Change in Clinicians Behavior • Modeling Addictions with Discounting • Deconstructing “Impulsivity” • Decision Deficits in OCD • Decision Deficits in Pathological Gambling • Social Phobia and Ultimatum Game • Conjectures on the Nature of the Anxiety-Avoidance Relationship
Outline of Talk I I Introduction: Suicidal Behaviors, Ideation and Decisions II Mathematical Modeling, Translational Research, and Transdisciplinary Research • Comparing animal models to mathematical models • Why Decision Science should care about suicide ( and other aspects of psychopathology). • Why Psychiatrists should care about Decision Science III The Research Agenda of the Neurobiology of Suicide IV Towards a decisional (formal) model of suicidal behaviors A. Mixed Strategy Model of Suicide Behavior B. Adding Inter-temporal Choice and Future Discounting – a Markov Model C. Signaling Game Model – Modeling the Relationship Aspects of Some Suicidal Behaviors
Outline of Talk II V Lessons from Suicide Modeling • Theoretical Framework for suicidology • Alternative frame for analyzing existing data • Source of alternative operationalizations of key concepts and risk factors in suicidology and Other aspects of Psychological Dysfunction VII Taking Decision Making and Decision Science Seriously VII Future Directions • With Peter Jensen – Applying Decision Science to Dissemination of guidelines • With Randall Marshall – Applying Decision Science to Dissemination of CBT for PTSD Personal Journey • With Robert Rogers, Randall Marshall, Frank Schneier, Blair Simpson – Risk Perception and Decision Tasks in Anxiety Disorders
Suicidal Behviors • Completed Suicide: Rates about 3/100,000/ Year in US = 30,000/Year • Suicide Attempt 10-100 times more common than Completed – The ER Nightmare –Major Source of Mortality in Psychiatric Practice • Suicidal Preparation (Hoarding Pills): Rates Unknown • Suicidal Intent w/o Preparation: Rates Unknown • Suicidal Ideation – Quite Common, some estimates are 20% of young adults • The vast majority of suicides have seen a clinician within the months preceding the suicide • Yet, despite extensive research programs, predicting suicidal behavior has been an elusive goal
Risk Factors for Suicide I • Suicidal Thoughts and Behaviors • Suicidal Ideas, Plans, Attempts (current or past) • Suicidal Intent • Lethality of Plans or Attempt • Psychiatric Diagnosis • Physical Illness • Psychosocial features • Loss of Social Support • Unemployment ( Recent Loss of Job) • Drop in Socioeconomic Status • Poor Family Ties • Domestic Violence • Other Life Stressors
Risk Factors for Suicide II • Childhood Trauma • Sexual or Physical or Psychological Abuse • Genetic Familial Factors • Family History of Suicide ( see Hemingways) • Family History of Mental Illness • Psychological Features • Hopelessness • Psychic Pain • Severe Anxiety • Panic Attacks • Shame or Humiliation • Psychological Turmoil • Loss of Self Esteem • Narcissistic Vulnerability • Agitation • Impulsivity • Aggression
Risk Factors for Suicide III • Cognitive Features • Executive Function Impairments • Thought Constriction ( Tunnel Vision) • Polarized Thinking Style • Closed Mindedness • Demographic Features • Male Gender ( But see New York City Police) • Widowed, Divorced or Single ( Especially for men) • Adolescents are group with highest number of suicides (Third Leading Cause of Death In 15-19 Year-olds, After Accidents and Homicides., 7.4 /1000,000/Yr, = 1,500 Deaths per year in US • White Race ( BUT See Police) • Gay, Lesbian, or Bisexual Orientation • Other Features • Access to Firearms • Intoxication • Substance Abuse • Protective Features • Children in Home or Responsibility to Family ( Except for Post Partum MDD) • Pregnancy ( Except post-partum depression/psychosis) • Religiosity • Life Satisfaction • Reality Testing • Positive Coping Skills / Problem Solving Ability • Social Support • Therapeutic Relationship / SOMATIC ANXIETY
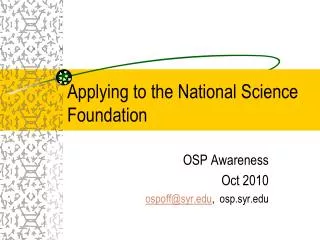
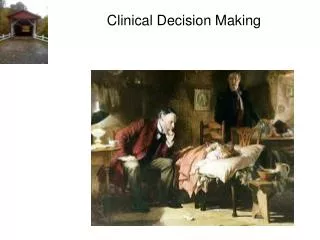
The Prediction Problem - I p1 Non Suicide Ideator Suicide Ideator p2 Low Lethality Attempter p10 p3 p1 p8 p1 p1 p1 p1 p1 p9 p5 p4 p6 High Lethality Attempter Suicide Completer p7
The Prediction Problem -II • Clinicians deal with ideators and attempters and need to predict probability of transition to attempter status or completer status in future. • Only a small fraction of ideators actually make an attempt. P2 <<< 1 and P9 <<< 1. Only a fraction of attempters complete suicide. P7 < 1 and P4 << 1. • Perhaps only high-lethality attempters are at high risk for completion – accidents excepted. • The risk relationships between these behaviors is not that clear BECAUSE THERE IS NO BEHVIORAL THEORY TO GUIDE RESEARCH
Why Psychiatric Suicidologists Should Care to Study Rational Choice Models • Decision making requires integrating basic capacities into an organized cognition/behavior – a decision (recall your mental experiences in the ultimatum game) • Yet decision making appears to be below the complexity level of clinical phenomena and thus a potential explanation for them e.g. a deficit in discounting may underlie addictive behaviors • Decision-making is at a complexity level between clinical phenomenon and basic neuro-bio-psychological functional modules.
Why Psychiatric Suicidologists Should Care to Study Rational Choice Models • Because of its unique place in the hierarchy of behavioral complexity – more complex that most basic neuropsych functionalities we usually measure but less complex than clinical symptoms- decision making involves interactions of simpler systems , anatomical, neurochemical, and psychological • As the following talks will show decision making concepts appear to map nicely onto the interaction of these anatomical, pharmacological as well as cognitive structures allowing for experimental work in imaging, pharmacologic manipulation of behavior, and contextual manipulation of cognitive processes • In other words its good way to use our currently available research toys… tools.
Why Psychiatric Suicidologists Should Care to Study Rational Choice Models • The work of Kahneman and Tversky on judgment and decision anomalies (among normals) was only possible once a highly developed normative theory was in place against which to test human behavior • Similarly with emotional components of decision making which are now being incorporated into decision science. • These aren’t failures but serial successes of the research program • It is also important to note that rational choice axioms don’t preclude seemingly irrational behavior once there are two people involved as in the Prisoners Dilemma. • Rational choice need not lead to intuitively ‘sensible’ behaviors- In humans even the (axiomatically) rational s irrational
Why Decision Science Should Study Suicide and its Models • Important Public Health Problem in Its Own Right • End of Life Decisions – Health Care policy • Healthcare doesn’t work in America • Costs of Cars’ steel vs. Healthcare and outsourcing • End of Life Costs a Major Factor • End of Life Decisions – Bioethics • Wedge Issue Similar to Abortion • Life Boundary Issues – Beginning, End, Ownership and Right
Why Decision Science Should Care to Study Suicide and Its Modeling • Rational Choice Modeling of Suicide and Related Questions of Determining a Utility Function for Life Itself • One’s most Valued Commodity • Greatest Liability • Capital Asset • Production Function • Individual Marketplace • Integrated Discounted Consumption Basket • Meaning/Signal Based Value Assessment • Contextual Specific Signal / Values / License • Moral High ground • License to Kill
Why Decision Science Should Care to Study Suicide and Its Modeling • The Dynamics of Spending or Risking Life in Political Marketplace • Almost Never see this in Economic Marketplace Exception: Life insurance, Suicide • When does one spend Life, or appear to, and what does it buy (Castro in the Mountains) • Willingness to die as a license to kill
Why Decision Scientists Should Care to Study Suicide and its Models • Meaning / Signal Based / Licensing and Value Assessment • Contextually Specific Values • Moral Currency Not Quite the High ground • Is a Uniform a License to Kill • Is willingness to die without uniform a license to kill • Uniformed vs. Clandestine ( when is uniform advantageous) • Target Civilian vs. Combatant vs. Both • Risky Missions vs Suicide ( do S justify lack of uniform /civilian target?) • Symmetric Information vs. Asymmetric • Relate to Notion of Asymmetric War and Asssymetry of material forces • For Whom is The Signal ( Signals) Intended • Communal Induction of Strategic Emotion • Community as Suicides antitheses reversal for suicide bombers
Research Agenda for Neurobiology of Suicidal Behaviors Suicidal Behaviors Operationalized (Psychometric) Behavior and cognitions related to suicidal risk Beck Depression Scale Impulsivity Scale Hopelessness Scale etc. Biological Factors Neuro-chemical Anatomical Etc Basic Modular Neuropsychological Functions
Role of Decision Science for Neurobiology of Suicidal Behaviors Suicidal Behaviors Behavior and cognitions related to suicidal risk Beck depression Impulsivity Hopelessness etc. Biological Factors Neuro-chemical Anatomical Etc Rational Choice Models “neuro-economics” Basic Neuropsychological Functions
Expanded Stress Diathesis Model: Incorporating a Decisional Axis
What Decision Science has to Offer:Decision Modeling • Formal Modeling offers a framework for conceptualizing an area of behavior as well as a ‘normative” model, both of which generate empirically testable questions: Rational Choice Models have made the Study of Bias, Heuristics, and Emotions Possible • Formal Modeling suggests alternative operational-ization of key cognitive concepts and behavioral tendencies • Formal Modeling offers alternative approaches to analyzing existing data
Decision Theory Modeling • This study aimed at developing models based on Game Theory that would incorporate what is known about suicidal risks and behaviors • Explanatory • Unifying • Predictive • Hypothesis Generating
“Economic” Modeling of Suicide • The real definition of originality • Darwinian model (deCatanzaro, 1986) • Cost-Benefit analysis (Yeh et al, 1987) • Demand Supply model (Yang et al, 1996) • Labor Force model (opportunity set?) (Huang, 1991) • Investment under uncertainty (Dixit et al, 1994) • Game theory model – suicide as signaling behaviors (Rosenthal, 1993) • Strategic Suicide (Norberg et al, 2000)
Naïve Expected Utility Model U (Status quo) Decision U (Death) Where U(X ) = The subjective Utility of a state
Mixed Strategies Model • Nash equilibrium based on need for Mixed Decision Strategies • The idea of mixed strategies is that sometimes the only good response to uncertainty is even more uncertainty, deliberate uncertainty. • Examples Menu Coalitions, Balanced portfolio, Coin toss • Key insight: The real decision is whether to make an attempt. This is a decision under uncertainty.
Mixed Strategy Model U(Status Quo) No Attempt U(New Status) Decision p(Death) ~ f (Attempt lethality, and /or Intent) Attempt U(Death)
Mixed Equilibrium Model • The “solution” is a mixed strategy in which dying and surviving are both seen as possible outcomes with varying probabilities. • In formal terms this is high stakes lottery. • FORMAL MODEL OF AMBIVALENCE • The decision maker (DM) chooses an attempt with a particular probability parameter – namely the lethality of the attempt. • “Nature-Chance” then dictates the actual outcome --state of affairs. • For now we assume that the utilities are independent of the probability.
Mixed Equilibrium Model U(Status Quo) No Attempt U(New Status) Decision p(Death) ~ f (attempt lethality) Attempt U(Death)
Mixed Equilibrium Model • The utility of not attempting suicide is U(SQ). • The Expected Utility (EU) of attempting suicide with lethality p is weighted average of surviving and dying EU = pU(d)+(1-p)U(NS) • The DM will attempt suicide whenthe probability of Death p0 is such that U(SQ) < p0U(D)+(1-p0)U(NS) • The question is, when will that be the case?
Implications of the Model I • While the naïve model allows for only two cases • U(D) < U(SQ) or U(SQ) < U(D) • The current model implies six cases • Three for U(D) < U(SQ) – “No Death Wish” • U(D) < U(NS) < U(SQ) -- Normal -- Not an attempter • U(NS) < U(D) < U(SQ) -- Samurai -- Not an attempter • U(D) < U(SQ) < U(NS) -- “manipulative” -- Only low lethality
Implications of the Model II • Three for U(SQ) < U(D) - “Death Wish” • U(SQ) < U(D) < U(NS) -- Desperation -- Prefers Low lethal • U(NS) < U(SQ) < U(D) --Cautious Terminal -Only high lethal • U(SQ) < U(NS) < U(D) --Hopeless --Prefers high lethal
Implications of the Model III • Consider U(D) < U(SQ) < U(NS): --“the manipulative gesture” • The indifference point p0 is given by: p0= [U(NS) - U(SQ)] / [U(NS)- U(D)] • [U(NS) - U(SQ)] is the potential utility gained from surviving an attempt. Call this the Gain, which is a positive quantity • [U(NS)- U(D)] = {[U(NS) – U(SQ)] + [U(SQ) – U(D)]} • [U(SQ) – U(D)] is the current perceived Value of Living (VoL) which is positive.
Implications of the Model IV • Thus to “take the gamble” • p0 <= Gain______ Gain + VoL • The quantity above depends on the relative perceived worth of Gains compared to current VoL. • In general this DM makes only low lethality attempts. • But depression (decrease in VoL) or neediness (increase in Gains) will increase acceptable lethality .
Implications of the Model V • The difference U(SQ) – U(D) is not by itself predictive of attempt. The literature bears this out as severity of depression does not correlate well with attempter status • Risk of an attempt depends on U(NS) a factor rarely elicited in suicide risk assessment • The lethality level chosen depends on U(NS). The model predicts that the availability of a method ( of a particular lethal potential) is extremely important in determining if an attempt occurs, as borne out in the literature. • FORMAL MODEL OF LETHALTY INTENT LEVEL • Thus, prevention strategy is type dependant -- e.g. removing firearms -- may not help for the wrong type
Implications of the Model VI • This DM prefers status quo to death but is willing to risk death at some level to arrive at a desired post attempt state. (like Army volunteers). This could be a change in status in family relations in financial or legal situation it could be a desired hospitalization. • In this case the attempt will be limited to low lethality methods, as is found in certain adolescents who make dramatic but low lethal attempts in order to influence a situation about which they feel they are helpless to change in any other way.
Implications of the Model VII • Risk assessment is often done on basis of estimates of patients wish to die instead of their willingness to make an attempt. • Yet this model indicates that some of the truly suicidal will not make an attempt unless the correct lethality level is available. • Similarly, some non-suicidal will make an attempt under right conditions.
Implications of the Model VIII Model predicts that one could reduce risk in “manipulative” type by reducing U(NS) this is consistent with Kernberg's contracting of the therapeutic frame in which specific disincentives are part of the therapy for this specific patient type. This may be the basis for clinical practice of “contracting for safety” with suicidal patients
Markov Model • This previous model assumes that the Status Quo is permanent. • A more realistic model must include the fact that patients status changes, and they have some expectation of the possibility of this change— • Hope and its opposite Hopelessness
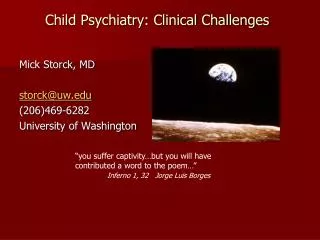
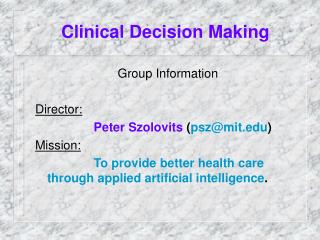
The Markov Model P(r) P(s) Depressed State Recovery P(t) P(w)
Markov Model • This introduces three new parameters, the first is p(R) perceived probability of recovery -- • The second is the degree of expected recovery reflected in the Utility of recovery. • Third is discount rate on future well being • Taken together these may correspond to measurements of hopelessness that strongly correlate with suicidal status … • FORMAL MODEL OF HOPLESSNESS
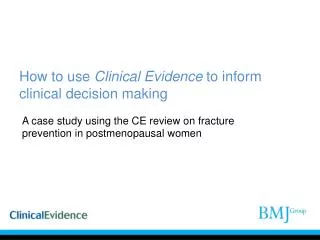
Markov Model U(R) Recovery Recovery }n { {<<} p(R) No Attempt SQ U(NS) p(D) Attempt U(D)
Markov Model • The third parameter relates to when one expects to recover. • How long will it take? • Can I hold on? • This introduces a discounting factor which may relate to degree of impulsivity in suicidal behavior – (a well established risk factor). • FORMAL MODEL OF IMPULSIVITY
Markov Model • Closely related to this is an unexpected bonus that fell out of this model, namely the protective effect of future potential attempts. • “Suicidal thoughts have gotten me through some bad nights” Nietzsche • The only thing that keeps me from attempting suicide is that I could do it tomorrow –and I hold on one day at a time (Patient comment). • Suicide attempt are “at the margin”.
Signaling Game Model • Question –In the case of a “manipulative’ attempt (we don’t like this word) doesn’t the DM have to take into account the reaction of others? • Might That reaction not depend on the nature and lethality of the attempt? • Signaling games are a class of games that have been studied that precisely model this attempt situation • As a benefit it help us get rid of the word ‘manipulative’ • Unless you want to grant that all signaling games including dressing well for an interview are also ‘manipulative’.
Signaling Game ModelL. Amsel, 2001 Recovery {<<} }n { U(R) Recovery U(NS-L) Status Quo U(NS-H) Attempt Low (Nature) pL (D) U(D) Attempt High U(NS-L) pH (D) U(NS-H) (copy of above for another type)