Download
1 / 58
580 likes | 790 Views
Roadmap to Emerging Regions: Clinical Trials in Developing Countries. International Clinical Trials Conference New York, 26 February 2009 Written By: Cristiana Spontoni Partner Squire, Sanders & Dempsey L.L.P. Brussels Presented by: Michael A. Swit, Esq. Vice President

E N D
Roadmap to Emerging Regions: Clinical Trials in Developing Countries International Clinical Trials Conference New York, 26 February 2009 Written By: Cristiana Spontoni Partner Squire, Sanders & Dempsey L.L.P. Brussels Presented by: Michael A. Swit, Esq. Vice President The Weinberg Group Inc. San Diego, California
The Global Landscape 69,175 clinical trials are being carried out in 161 countries1 • Increasingly being conducted in Central & Eastern Europe, Latin America and Asia Majority of trials are conducted in the U.S. and Western Europe Trials increasingly outsourced to Clinical Research Organizations
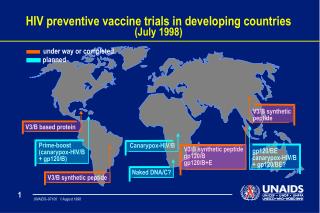
Globalization of Trials: European Data According to the EMEA, around one quarter of patients recruited in pivotal trials submitted in MAAs to EMEA between 2005 and 2008 were recruited in: Latin America Asia CIS Africa
Recurrent Themes in Global Trials Good central coordination but flexibility to local requirements/habits/culture (eg, CTA templates) Sound use of resources: CRO, PIs, Sites: how much should be delegated and how much should be kept under control (eg, negotiating/entering CTAs, filing for regulatory approvals) All the more true in emerging economies…
Advantages Of Emerging Economies Limited costs: drugs, hospitalisation, travel and other general expenses, basic support services Higher number of patients, especially naive patients (i.e., patients who never received a treatment) Large patient populations with diseases of both developed and developing countries (e.g., HIV/AIDS) Multi-ethnic/multiracial populations Wide spectrum for diseases Potential new markets (e.g., China) Competent/motivated PIs
Conducting trials in emerging regions poses a number of challenges: Different treatments and standard of care Differing levels of clinical research experience and sophistication Different capabilities of CROs in the region Requires greater direct management efforts Many apparent similarities in challenges requiring different responses Clinical Trials in Emerging Regions
Regulatory Trial Designs Regulatory Authorities and IRB/ECs Translation requirements Import/Export licenses Legal Contracts/Clinical Trial Agreements Insurance requirements Intellectual property issues Other CRO Partnering Site/Investigator Identification Adherence to Good Clinical Practice Assuring the Ethical Conduct of the Trial Quality Control issues Cultural and infrastructure considerations Challenges of Conducting These Clinical Trials
An ordinary day in an ordinary global trial-- Some real life experiences --
Practical Challenge: Control of Temperature “Control of storage and transportation temperatures is essential in maintaining the quality of medicines and in helping to protect patients from sub-standard or ineffective medicines that may result from inadequate control” (J. Taylor, Quality and Standards Manager, MHRA) Increased risks for biotech products, vaccines, blood products, semi-solids, chemically unstable at certain temperatures, and of course, study drugs.
Let’s Get a Fridge! Sponsor wants to perform a study at site x Site x does not have a way of keeping Study Drug at appropriate controlled temperature Let’s get a fridge there! OK BUT… Can sponsor sell/donate the fridge? To whom? Under what circumstances? Do we need a written contract? Do we need to get prior authorizations? From whom? What if Site is a public hospital? What if we are talking about very expensive medical devices? Can the fridge be imported in country x?
Legal Challenge: Study in 21 Jurisdictions in the EMEA Region Can a CTA be entered by a non-local Sponsor? Answer:- Yes, BUT -- in one jurisdiction, still need to go through local entity or mediator- Yes BUT -- in Israel, sites often will object to contracting with a non-Israeli entity- Yes BUT -- certain regulatory procedures will have to be performed by local entities either because it is required by law (e.g., Ukraine) or because -- that’s the way we do things here (Middle East)
Legal Challenge 2: What’s the Right Price? Sponsor sells x vials of Study Drug to a non EU European country Custom authorities google name of Study Drug and find its price in the US: 10,000 USD Custom authorities apply a custom duty considering that value of the Study Drug Should Sponsor pay? What’s the practice in other countries?
Ethical Challenge: Unusable Data Violations result in unusable data: in requesting marketing authorisation, a company submits a file to the EMEA, which includes the description of the trial performed. In examining the file, the EMEA evaluates the respect of GCP, the granting of informed consent and the approval by ECs. Illustrates just how important compliance with GCP will be
The Rules in Emerging EU Jurisdictions Estonia, Hungary, Latvia, Lithuania, Czech Republic, Slovakia, Slovenia, Poland, Bulgaria, Romania, Malta, Cyprus: now all EU countries Directive 2001/20/EC on clinical trials applies: - GCP standards- Uniform regulatory requirements- BUT: local challenges still remain Highly educated and competent investigators
The EU Directive on Clinical Trials Same rules (in principle!) across 27 jurisdictions Commercial + Non-commercial trials Phases I,II,III,IV All trials except “non-interventional” trials
Industry, Government, Research Council, University, … Does not need to be EU-based but must appoint EU-based representative that bears civil and criminal liability as EU-based sponsors Sponsor can delegate (NOT transfer!) sponsor responsibilities to third parties (e.g., CROs) BUT sponsor bears ultimate responsibility The Sponsor
Informed consent Special consideration for children and incapacitated adults Data protection: Directive 95/46/EC regulates strictly any processing or transfer of data outside the EU Medical data qualifies as “sensitive” The US is considered not a “safe place” for the purpose of data protection Protection of Trial Subjects
Commencement of Trials in the EU 60 days max 1 x clock stop for info. 60+30+90 days max No Time Limit (exception) Sponsor applies for EUDRACT number Application to EC Notification to CA CA no grounds for non-acceptance Explicit authorization required only in certain cases Favorable Opinion of EC Separate procedures but can run in parallel One opinion per MS
Substantial amendments to be notified to ECs and CAs (35 days max) Safety measures adopted to protect safety of subjects Notification of trial end (90 days or 15 if early termination) Notification of SUSARs fatal or life threatening: 7 days other SUSARs: 15 days annual reporting Notification of Serious Adverse Events Guidance on reporting and standard forms Conduct of a Trial – Reporting Obligations
Manufacture/importation authorisation Authorisation holder must have QP at disposal: check compliance with EU GMPs or standards that are “at least equivalent” IMPs must be supplied free of charge IMPs – Investigational Medicinal Products
CAs can suspend or prohibit trials if: conditions for granting authorisation for trial conduct are not met anymore doubts about safety/scientific validity Must consult with sponsor/investigator except in cases of “imminent risk” CA will inform other CAs, EMEA and European Commission You may have duty to inform FDA as well Suspension of Trials - Infringements
Before, during or after completion of a trial As part of marketing authorisation process or follow-up to it At: trial sites, IMP manufacturing site, any laboratory used in the trial, or at sponsor’s premises Conducted by CAs Inspections on GCP/GMP Compliance
GCP Violations = Unusable Data Drugs reviewed by the EMEA can be granted a marketing authorization only if they are based on clinical trials conducted in compliance with the Declaration of Helsinki In requesting marketing authorisation, a company submits a file to the EMEA, which includes the description of the trial performed. In examining the file, the EMEA evaluates the respect of GCP, the granting of informed consent and the approval by ECs. When problems are identified, namely regarding ethical aspects, the EMEA can advise the Commission to refuse the marketing authorisation or can advise the withdrawal of marketing authorisation already delivered by Member States. This information is also made public. However, the EMEA intervention happens after the clinical trial is finalised and presented in the file and not before or during the trial.
Inconsistent Approach/Interpretation An example… Question: can sponsor be non-EU based? EU law answer: yes, if it appoints a EU-based representative Answer in BG, Czech Rep., Estonia, Latvia, Lithuania, Malta, Romania, Slovakia, Slovenia: yes, if it appoints an EU representative Answer in Cyprus: NO!
EU Rules on Trials in Third Countries Financial penalties apply in case of failure to comply with clinical trials requirements Sites in third countries can be inspected by the competent authorities of Member States. The EMEA has a system of GCP inspections in third countries since 2006 which has led to an increasing number of inspections in Latin America, Africa and Asia Inspections concentrate primarily on: informed consent and appropriate EC (IRB) approvals EU assisting on GCP capacity building/inspections a number of countries - in last EMEA GCP Inspectors’ WG workprogramme: Croatia, Macedonia, Turkey
Increased Regulatory Scrutiny A European Commission paper of 2002 indicated that: The regulatory framework for clinical trials is expected to adapt to the globalization. the budget and number of international/national GCP inspectors is expected to increase more information on all these clinical trials should be available through an international database the key role of IRBs and of capacity building in this area
Opinion 17 of the European group on ethics in science and new technologies to the European Commission: “Ethical aspects of clinical research in developing countries” (February 2003) 2006-2008: Series of Parliamentary Questions on trials in poor countries On 5 December, the EMEA issued a strategy paper on: “Acceptance of clinical trials conducted in third countries for evaluation in Marketing Authorisations” Increased Regulatory Scrutiny …
EMEA Action Plan: Watch This Space! Three-year-s action plan includes: Clarify application of ethical standards Consider issues driving recruitment of subjects in third countries Consider tools to respond to non-compliance/step up GCP inspections Training of EMEA/sponsors/experts Increased transparency: EPAR should include a clear description of the assessment of ethical standards of trials in emerging economies Promote capacity building also through EU funding instruments
Wrap-Up Clear opportunities ahead of sponsors in emerging regions Require strong central coordination and resource management But, also must understand need for flexibility in approach and understanding of local specificities Beware of compliance pitfalls no matter where you conduct your trial!
Thanks!! Cristiana Spontoni, Partner T: 011.322.627.11.05 E: cspontoni@ssd.com
Roadmap to Emerging Regions: Sponsor Experiences in Central Europe and AsiaCarlos F. PezaFebruary 26, 2009
Recent Experiences in Emerging Regions • Phase IV trial in Oncology conducted in • 5 countries (France, Germany, Greece, Italy, Slovenia) • 250 sites • 8,448 valid subjects (3,719 valid controls) • Field period from November 2005 to October 2008 • Cross-Sectional Survey on Tobacco Prevalence in Indonesia • Inclusion criteria similar to control inclusion criteria in European study • 11 sites • 1,500 valid subjects • Field period from January to October 2007 • Research was financially supported by Philip Morris International
Why Slovenia? • Small number of sites provided access to almost every subject in the country who was suffering from the target condition • Regulatory Agency and Central Ethics Committee are among the most efficient in Europe • Highly educated and motivated Investigators • Local CROs charged competitive fees for their services • Relatively few challenges for study start up and conduct
Specifics of Slovenian Situation • Small country, well reachable • Centralized healthcare system with developed referral network • Approximately 100 clinical trials are performed annually • Laws and regulations for conducting clinical trials are based on EU Clinical Trials Directive (2001/20/EC) • Agency for Medicinal Products and Medical Devices (JAZMP) is the competent authority for clinical trial authorization • EC approval given at the national level by the National Medical Ethics Committee • National Cancer Registry
Overcoming the Challenges in Slovenia • Challenge: Identifying and vetting the appropriate CRO • Identify the strength and weaknesses of potential vendors • Understand how you will have to supplement for the potential weaknesses • Our approach: • Vetted international and national CROs • Decided on National/Local CRO • Identified its strengths • Worked with them to shore up their potential weaknesses
Overcoming the Challenges in Slovenia • Challenge: Obtaining ethics approval for a controversially funded study • Our approach: • Recruited Principal Investigator wisely • Provided him with the information needed to fully understand and promote the study • Became invested in the study • Good reputation, leadership skills, and willing to act as a key advocate of the study • Set the stage with Ethics Committee • Identified, recruited and developed good working relationship with Key Opinion Leaders in order to understand local considerations • Understood the potential concerns of the members • Addressed these during the submission • Gained support of stakeholders and who demonstrated this support to EC
Overcoming the Challenges in Slovenia • Challenge: Achieving potential subject recruitment • Our approach: • Developed Principal Investigator and sub-investigators as key promoters and coordinators • Coordination and promoting activities of different sites • Coordinating and promoting study within site • Developed investigator network where subjects were identified in the periphery and “treated” in the central location • Motivated site team • Actively recognize the role of each site member • CRA partnership with sites • Kept site team informed and involv
Slovenian Participation in the Study • 1 Local/National CRO • 16 Sites • 1 Country Principal Investigator, 24 investigators/subinvestigators, more than 20 study nurses • Comparably high recruitment rate • First patient in: April 2007 • 1,391 valid subjects (721 valid controls) • 16% of total study subjects recruited within one year • Recruitment rate stable over the year (no holiday gaps)
Our Experience in Slovenia • Excellent experience in Slovenia • High subject recruitment rate • Qualified and motivated medical professionals • Uniformed regulatory issues as in Western Europe • EU Clinical Trials Directive, ICH and GCP already implemented • Relatively lower CRO costs to conduct the trial
Indonesian Smoking Prevalence Study • Originally intended to conduct a series of studies to understand the relative risks of smoking for a several disease end point • Planned to conduct several case-control studies for each of the disease endpoints • In planning the studies, it was determined that there did not exist valid epidemiological data to be able to guide the design of the studies • A pilot study of patients in hospitals to be used in the case-control studies was conducted
Specifics of the Indonesian Situation • Large Country • Very few trials being conducted, but numbers are growing. • Government and investigators receptive to industry knowledge • GCP implemented into national laws and guidelines governing clinical trials • ECs to be established at institutional, regional/provincial, and national levels according to need • National Agency for Drug and Food Control is competent authority for clinical trial authorization • Lack of population-based registries • Hospital based-cancer registries in 13 cities
Indonesian Smoking Prevalence Study • Cross-sectional study on the smoking prevalence of Indonesian male hospital patients • Study performed to regulated standards of a clinical trial • 11 hospital sites in Jakarta, Solo, Surabaya, Padang • 1 Principal Investigator, 22 investigators/subinvestigators, 60 CRA/interviewers • More than 18,000 medical records evaluated • 1,533 valid subjects recruited • 38 week field period
Overcoming the Challenges in Indonesia • Challenge: Designing a clinical trial to account for the specifics of the region • Cultural issues • Inclusion/Exclusion Criteria • Trial Length and approval timings • Infrastructure issues • Investigator and Staff Training • Our approach: • Trial designed to account: • Differences in medical practice (disease diagnosis, investigator-patient relationship) • Translation of study/regulatory documents • Validation of measurement scales (patient questionnaire) • Understood need to apply “partnership approach” to build supportive relationships