Download
1 / 1
10 likes | 118 Views
Malocclusions and Urolithiasis in the Context of Evolutionary Medicine Libertini G. (M.D., Independent Researcher). 1. 2. 3.

E N D
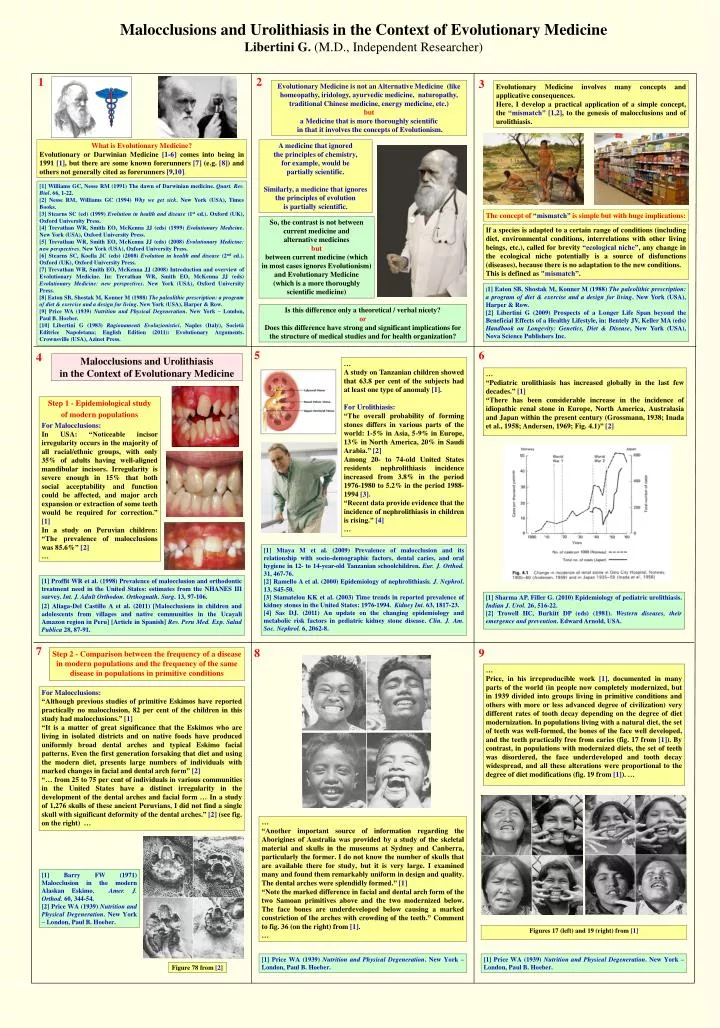
Malocclusions and Urolithiasis in the Context of Evolutionary Medicine Libertini G. (M.D., Independent Researcher) 1 2 3 Evolutionary Medicine is not an Alternative Medicine (like homeopathy, iridology, ayurvedic medicine, naturopathy, traditional Chinese medicine, energy medicine, etc.) but a Medicine that is more thoroughly scientific in that it involves the concepts of Evolutionism. Evolutionary Medicine involves many concepts and applicative consequences. Here, I develop a practical application of a simple concept, the “mismatch” [1,2], to the genesis of malocclusions and of urolithiasis. What is Evolutionary Medicine? Evolutionary or Darwinian Medicine [1-6] comes into being in 1991 [1], but there are some known forerunners [7] (e.g. [8]) and others not generally cited as forerunners [9,10]. A medicine that ignored the principles of chemistry, for example, would be partially scientific. Similarly, a medicine that ignores the principles of evolution is partially scientific. [1] Williams GC, Nesse RM (1991) The dawn of Darwinian medicine. Quart. Rev. Biol. 66, 1-22. [2] Nesse RM, Williams GC (1994) Why we get sick. New York (USA), Times Books. [3] Stearns SC (ed) (1999) Evolution in health and disease (1st ed.). Oxford (UK), Oxford University Press. [4] Trevathan WR, Smith EO, McKenna JJ (eds) (1999) Evolutionary Medicine. New York (USA), Oxford University Press. [5] Trevathan WR, Smith EO, McKenna JJ (eds) (2008) Evolutionary Medicine: new perspectives. New York (USA), Oxford University Press. [6] Stearns SC, Koella JC (eds) (2008) Evolution in health and disease (2nd ed.). Oxford (UK), Oxford University Press. [7] Trevathan WR, Smith EO, McKenna JJ (2008) Introduction and overview of Evolutionary Medicine. In: Trevathan WR, Smith EO, McKenna JJ (eds) Evolutionary Medicine: new perspectives. New York (USA), Oxford University Press. [8] Eaton SB, Shostak M, Konner M (1988) The paleolithic prescription: a program of diet & exercise and a design for living. New York (USA), Harper & Row. [9] Price WA (1939) Nutrition and Physical Degeneration. New York – London, Paul B. Hoeber. [10] Libertini G (1983) Ragionamenti Evoluzionistici. Naples (Italy), Società Editrice Napoletana; English Edition (2011): Evolutionary Arguments. Crownsville (USA), Azinet Press. The concept of “mismatch” is simple but with huge implications: So, the contrast is not between current medicine and alternative medicines but between current medicine (which in most cases ignores Evolutionism) and Evolutionary Medicine (which is a more thoroughly scientific medicine) If a species is adapted to a certain range of conditions (including diet, environmental conditions, interrelations with other living beings, etc.), called for brevity “ecological niche”, any change in the ecological niche potentially is a source of disfunctions (diseases), because there is no adaptation to the new conditions. This is defined as "mismatch”. [1] Eaton SB, Shostak M, Konner M (1988) The paleolithic prescription: a program of diet & exercise and a design for living. New York (USA), Harper & Row. [2] Libertini G (2009) Prospects of a Longer Life Span beyond the Beneficial Effects of a Healthy Lifestyle, in: Bentely JV, Keller MA (eds) Handbook on Longevity: Genetics, Diet & Disease, New York (USA), Nova Science Publishers Inc. Is this difference only a theoretical / verbal nicety? or Does this difference have strong and significant implications for the structure of medical studies and for health organization? 5 6 4 Malocclusions and Urolithiasis in the Context of Evolutionary Medicine … A study on Tanzanian children showed that 63.8 per cent of the subjects had at least one type of anomaly [1]. For Urolithiasis: “The overall probability of forming stones differs in various parts of the world: 1-5% in Asia, 5-9% in Europe, 13% in North America, 20% in Saudi Arabia.” [2] Among 20- to 74-old United States residents nephrolithiasis incidence increased from 3.8% in the period 1976-1980 to 5.2% in the period 1988-1994 [3]. “Recent data provide evidence that the incidence of nephrolithiasis in children is rising.” [4] … … “Pediatricurolithiasis has increased globally in the last few decades.” [1] “There has been considerable increase in the incidence of idiopathic renal stone in Europe, North America, Australasia and Japan within the present century (Grossmann, 1938; Inada et al., 1958; Andersen, 1969; Fig. 4.1)” [2] Step 1 - Epidemiological study of modern populations For Malocclusions: In USA: “Noticeable incisor irregularity occurs in the majority of all racial/ethnic groups, with only 35% of adults having well-aligned mandibular incisors. Irregularity is severe enough in 15% that both social acceptability and function could be affected, and major arch expansion or extraction of some teeth would be required for correction.” [1] In a study on Peruvian children: “The prevalence of malocclusions was 85.6%” [2] … [1] Mtaya M et al. (2009) Prevalence of malocclusion and its relationship with socio-demographic factors, dental caries, and oral hygiene in 12- to 14-year-old Tanzanian schoolchildren. Eur. J. Orthod. 31, 467-76. [2] Ramello A et al. (2000) Epidemiology of nephrolithiasis. J. Nephrol. 13, S45-50. [3] Stamatelou KK et al. (2003) Time trends in reported prevalence of kidney stones in the United States: 1976-1994. Kidney Int. 63, 1817-23. [4]Sas DJ. (2011) An update on the changing epidemiology and metabolic risk factors in pediatric kidney stone disease. Clin. J. Am. Soc. Nephrol. 6, 2062-8. [1] Proffit WR et al. (1998) Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES III survey. Int. J. Adult Orthodon. Orthognath. Surg. 13, 97-106. [2] Aliaga-Del Castillo A et al. (2011) [Malocclusions in children and adolescents from villages and native communities in the Ucayali Amazon region in Peru] [Article in Spanish] Rev. Peru Med. Exp. SaludPublica 28, 87-91. [1] Sharma AP, Filler G. (2010) Epidemiology of pediatricurolithiasis. Indian J. Urol. 26, 516-22. [2] Trowell HC, Burkitt DP (eds) (1981). Western diseases, their emergence and prevention. Edward Arnold, USA. 7 8 9 Step 2 - Comparison between the frequency of a disease in modern populations and the frequency of the same disease in populations in primitive conditions … Price, in his irreproducible work [1], documented in many parts of the world (in people now completely modernized, but in 1939 divided into groups living in primitive conditions and others with more or less advanced degree of civilization) very different rates of tooth decay depending on the degree of diet modernization. In populations living with a natural diet, the set of teeth was well-formed, the bones of the face well developed, and the teeth practically free from caries (fig. 17 from [1]). By contrast, in populations with modernized diets, the set of teeth was disordered, the face underdeveloped and tooth decay widespread, and all these alterations were proportional to the degree of diet modifications (fig. 19 from [1]). … For Malocclusions: “Although previous studies of primitive Eskimos have reported practically no malocclusion, 82 per cent of the children in this study had malocclusions.” [1] “It is a matter of great significance that the Eskimos who are living in isolated districts and on native foods have produced uniformly broad dental arches and typical Eskimo facial patterns. Even the first generation forsaking that diet and using the modern diet, presents large numbers of individuals with marked changes in facial and dental arch form” [2] “… from 25 to 75 per cent of individuals in various communities in the United States have a distinct irregularity in the development of the dental arches and facial form … In a study of 1,276 skulls of these ancient Peruvians, I did not find a single skull with significant deformity of the dental arches.” [2] (see fig. on the right) … … “Another important source of information regarding the Aborigines of Australia was provided by a study of the skeletal material and skulls in the museums at Sydney and Canberra, particularly the former. I do not know the number of skulls that are available there for study, but it is very large. I examined many and found them remarkably uniform in design and quality. The dental arches were splendidly formed.” [1] “Note the marked difference in facial and dental arch form of the two Samoan primitives above and the two modernized below. The face bones are underdeveloped below causing a marked constriction of the arches with crowding of the teeth.” Comment to fig. 36 (on the right) from [1]. … • [1] Barry FW (1971) Malocclusion in the modern Alaskan Eskimo. Amer. J. Orthod. 60, 344-54. • [2] Price WA (1939) Nutrition and Physical Degeneration. New York – London, Paul B. Hoeber. Figures 17 (left) and 19 (right) from [1] • [1] Price WA (1939) Nutrition and Physical Degeneration. New York – London, Paul B. Hoeber. • [1] Price WA (1939) Nutrition and Physical Degeneration. New York – London, Paul B. Hoeber. Figure 78 from [2]