Download
1 / 1
10 likes | 103 Views
Evolutionary definition of disease phenomenon Libertini G. (M.D., Independent Researcher).

E N D
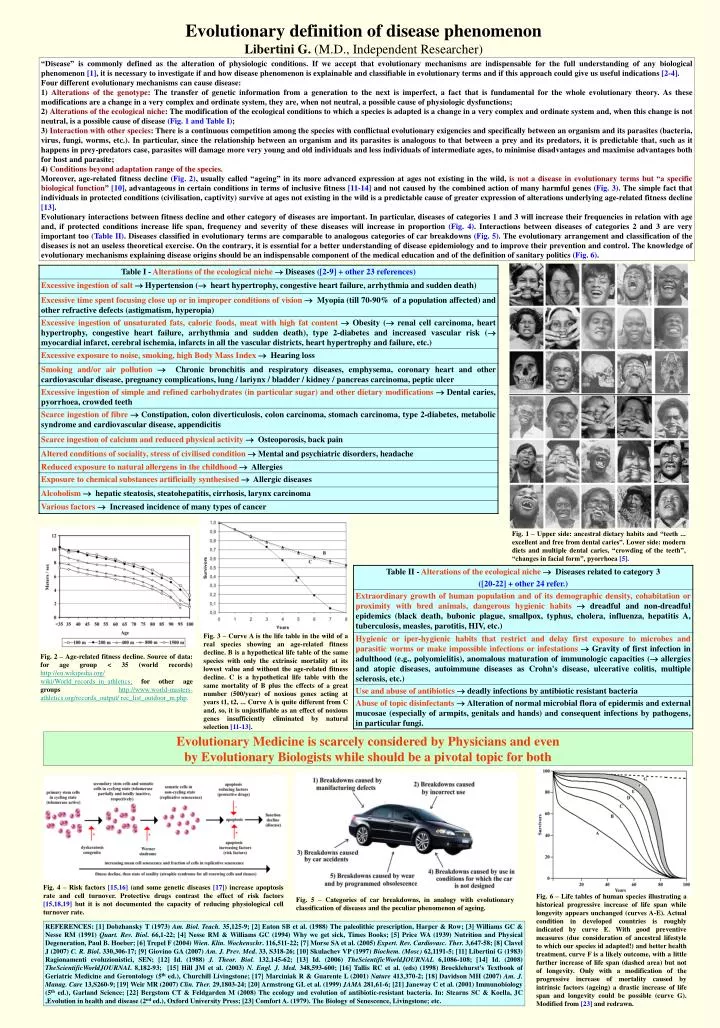
Evolutionary definition of disease phenomenon Libertini G. (M.D., Independent Researcher) “Disease” is commonly defined as the alteration of physiologic conditions. If we accept that evolutionary mechanisms are indispensable for the full understanding of any biological phenomenon [1], it is necessary to investigate if and how disease phenomenon is explainable and classifiable in evolutionary terms and if this approach could give us useful indications [2-4]. Four different evolutionary mechanisms can cause disease: 1) Alterations of the genotype: The transfer of genetic information from a generation to the next is imperfect, a fact that is fundamental for the whole evolutionary theory. As these modifications are a change in a very complex and ordinate system, they are, when not neutral, a possible cause of physiologic dysfunctions; 2) Alterations of the ecological niche: The modification of the ecological conditions to which a species is adapted is a change in a very complex and ordinate system and, when this change is not neutral, is a possible cause of disease (Fig. 1 and Table I); 3) Interaction with other species: There is a continuous competition among the species with conflictual evolutionary exigencies and specifically between an organism and its parasites (bacteria, virus, fungi, worms, etc.). In particular, since the relationship between an organism and its parasites is analogous to that between a prey and its predators, it is predictable that, such as it happens in prey-predators case, parasites will damage more very young and old individuals and less individuals of intermediate ages, to minimise disadvantages and maximise advantages both for host and parasite; 4) Conditions beyond adaptation range of the species. Moreover, age-related fitness decline (Fig. 2), usually called “ageing” in its more advanced expression at ages not existing in the wild, is not a disease in evolutionary terms but “a specific biological function” [10], advantageous in certain conditions in terms of inclusive fitness [11-14] and not caused by the combined action of many harmful genes (Fig. 3). The simple fact that individuals in protected conditions (civilisation, captivity) survive at ages not existing in the wild is a predictable cause of greater expression of alterations underlying age-related fitness decline [13]. Evolutionary interactions between fitness decline and other category of diseases are important. In particular, diseases of categories 1 and 3 will increase their frequencies in relation with age and, if protected conditions increase life span, frequency and severity of these diseases will increase in proportion (Fig. 4). Interactions between diseases of categories 2 and 3 are very important too (Table II). Diseases classified in evolutionary terms are comparable to analogous categories of car breakdowns (Fig. 5). The evolutionary arrangement and classification of the diseases is not an useless theoretical exercise. On the contrary, it is essential for a better understanding of disease epidemiology and to improve their prevention and control. The knowledge of evolutionary mechanisms explaining disease origins should be an indispensable component of the medical education and of the definition of sanitary politics (Fig. 6). Fig. 1 – Upper side: ancestral dietary habits and “teeth ... excellent and free from dental caries”. Lower side: modern diets and multiple dental caries, “crowding of the teeth”, “changes in facial form”, pyorrhoea [5]. Fig. 3 – Curve A is the life table in the wild of a real species showing an age-related fitness decline. B is a hypothetical life table of the same species with only the extrinsic mortality at its lowest value and without the age-related fitness decline. C is a hypothetical life table with the same mortality of B plus the effects of a great number (500/year) of noxious genes acting at years t1, t2, ... Curve A is quite different from C and, so, it is unjustifiable as an effect of noxious genes insufficiently eliminated by natural selection [11-13]. Fig. 2 – Age-related fitness decline. Source of data: for age group < 35 (world records)http://en.wikipedia.org/ wiki/World_records_in_athletics;for other age groupshttp://www.world-masters-athletics.org/records_output/ rec_list_outdoor_m.php. Evolutionary Medicine is scarcely considered by Physicians and even by Evolutionary Biologists while should be a pivotal topic for both Fig. 4 – Risk factors [15,16] (and some genetic diseases [17]) increase apoptosis rate and cell turnover. Protective drugs contrast the effect of risk factors [15,18,19] but it is not documented the capacity of reducing physiological cell turnover rate. Fig. 6 – Life tables of human species illustrating a historical progressive increase of life span while longevity appears unchanged (curves A-E). Actual condition in developed countries is roughly indicated by curve E. With good preventive measures (due consideration of ancestral lifestyle to which our species id adapted!) and better health treatment, curve F is a likely outcome, with a little further increase of life span (dashed area) but not of longevity. Only with a modification of the progressive increase of mortality caused by intrinsic factors (ageing) a drastic increase of life span and longevity could be possible (curve G). Modified from [23] and redrawn. Fig. 5 – Categories of car breakdowns, in analogy with evolutionary classification of diseases and the peculiar phenomenon of ageing. REFERENCES: [1] Dobzhansky T (1973) Am. Biol. Teach. 35,125-9; [2] Eaton SB et al. (1988) The paleolithic prescription, Harper & Row; [3] Williams GC & Nesse RM (1991) Quart. Rev. Biol. 66,1-22; [4] Nesse RM & Williams GC (1994) Why we get sick, Times Books; [5] Price WA (1939) Nutrition and Physical Degeneration, Paul B. Hoeber; [6] Trepel F (2004) Wien. Klin. Wochenschr. 116,511-22; [7] Morse SA et al. (2005) Expert. Rev. Cardiovasc. Ther. 3,647-58; [8] Clavel J (2007) C. R. Biol. 330,306-17; [9] Giovino GA (2007) Am. J. Prev. Med. 33, S318-26; [10] Skulachev VP (1997) Biochem. (Mosc) 62,1191-5; [11] Libertini G (1983) Ragionamenti evoluzionistici, SEN; [12] Id. (1988) J. Theor. Biol. 132,145-62; [13] Id. (2006) TheScientificWorldJOURNAL 6,1086-108; [14] Id. (2008) TheScientificWorldJOURNAL 8,182-93; [15] Hill JM et al. (2003) N. Engl. J. Med. 348,593-600; [16] Tallis RC et al. (eds) (1998) Brocklehurst’s Textbook of Geriatric Medicine and Gerontology (5th ed.), Churchill Livingstone; [17] Marciniak R & Guarente L (2001) Nature 413,370-2; [18] Davidson MH (2007) Am. J. Manag. Care 13,S260-9; [19] Weir MR (2007) Clin. Ther. 29,1803-24; [20] Armstrong GL et al. (1999) JAMA 281,61-6; [21] Janeway C et al. (2001) Immunobiology (5th ed.), Garland Science; [22] Bergstom CT & Feldgarden M (2008) The ecology and evolution of antibiotic-resistant bacteria. In: Stearns SC & Koella, JC ,Evolution in health and disease (2nd ed.), Oxford University Press; [23] Comfort A. (1979). The Biology of Senescence,Livingstone; etc.