Download
1 / 39
400 likes | 594 Views
Exercise and cancer . Professor Robert Thomas Consultant Oncologist Addenbrooke’s, Bedford Cambridge University NHS Trusts Cranfield University. The cancer problem. 1 in 3 population will get cancer 1 in 4 die Most common cause of death in young women.

E N D
Exercise and cancer Professor Robert Thomas Consultant Oncologist Addenbrooke’s, Bedford Cambridge University NHS Trusts Cranfield University
The cancer problem • 1 in 3 population will get cancer • 1 in 4 die • Most common cause of death in young women UK Ca breast 41,700 new women annually
Outcomes improving 2 million cancer survivors in the UK
Common symptoms and risk amoung cancer survivors • Hot flushes • Bone density • Poor sleep pattern • Secondary cancers • Bowel adhesions • Weight gain • Indigestion • Sore hands • Fatigue and tiredness • Mood, anxiety • Depression • Brain power and intellect • Poor appetite • Constipation • Blood clots (thrombosis) • Quality of life
Self help and lifestyle after Cancer “Teachable moment”
What is the evidence? Lifestyle and cancer news - Cancernet.co.uk
Exercise after Cancer Reduce risks and side effects of treatment Slow the growth of an established cancer Prevent relapse after initial therapy Improve overall chance of cure
Cancer Related Fatigue • 28 RCT and 2 meta analysis reduces the severity of fatigue • Supervised aerobic exercise programmes more effective. • Adverse events during exercise were extremely low Cramp and Daniel, 2008), Velthuis et al., 2009
Prostate Cancer Patients on hormones • Progressive resistance and aerobic training 20 wk • Improved muscle strength, • Functional performance • Balance in older men • Mood, depression • Metabolic syndrome (Adult Treatment Panel III criteria) • Abdominal obesity, High triglyceride, Hyperglycaemia Daniel et al. Medicine & Science in Sports: Vol 38; 12 - pp 2045-52 Segal et al JCO, Vol 27, No 3 , 2009: pp. 344-351 .;
Prostate Radiotherapy Late Toxicity and Lifestyle Study Robert Thomas Bedford, Addenbrookes, Cranfield Mea Holme Oxford University Madeleine Williams Bedford Hospital Patricia Bellamy Cranfield University Christine Steel MacMillan Cancer Relief Jervoise Andreyev Royal Marsden Hospital
Purpose • Do self help lifestyle factors correlate with late toxicity after radiotherapy? • Exercise • Smoking • BMI • Age
Methods 470 live men sourced on the Lantis RXT data base Referred from Bedford Hospital over 10 years 440 completed the study questionnaire (94%) Approached in Clinic or via post +/- telephone calls • Toxicity • Vaizey rectal toxicity score • NCI common toxicity score • Rectal bleeding • Erectile function • Urinary incontinence • Lifestyle • Smoking habits • BMI, age • General practice physical activity questionnaire
Results 8% (35) smokers 1% were underweight (BMI <18.5)36% normal weight (18.5-25), 38% over weight (25-29.9) 25% obese (>25%).
Results 58% inactive, 27% moderately inactive/active, 11% active 4% exercising more than 3 hrs a week
Lifestyle and cancer-mechanisms Initial DNA damage Continuing DNA damage, Hormonal environment Immunity Proliferation, de-differentiation, adhesion, apoptosis, angiogenesis, invasion, metastasis
Lifestyle & tumour progression 93 men with indolent prostate cancer Exercise (>20 mins brisk walking 6 days a week) Yoga, Vegan diet High soy and antioxidant rich intake Ornish, 2005 #92
PSA at 1 year • Exercise (>20 mins brisk walking 6 days a wk) • Yoga, Vegan diet • High soy intake Control - increase by 6% PSA 10% difference significant at P>0.01 Intervention - decrease by 4% Trial entry At one year Ornish D, et al The Journal of Urology, 2005. 174: p. 1065-1070.
Cellular growth • Intervention - 70% growth reduction • Control group – 6% growth reduction • 64% difference highly significant at P>0.001 • Those with largest PSA reduction had highest reduction Prostate cell lines Ornish D, et al The Journal of Urology, 2005. 174: p. 1065-1070.
Lifestyle / salicylate study A randomised double blind phase II study of lifestyle counselling and salicylate +/- dietary supplements in patients with progressive prostate cancer. Robert Thomas, Roger Oakes, Dr Simon Russell, Ms Madeleine Williams. Thomas, et al. NCRN Conference proceeding 2008 Journal of Food and Science March 2009
Prevent relapse after initial therapy Improve overall chance of cure
Nurse’s Health Study (Breast cancer) 5204 registered nurses, Breast cancer 1976 -2000 860 deaths (553 breast cancer) BMI at diagnosis = Overall survival = Breast cancer relapse (nonsmokers) Weight gain more than 0.5kg/m2 at 1yr (greatest if >2kg/m2) = Overall survival = Breast cancer specific survival Kroenke CH, et al JCO 2005. 23(7): p. 1370-1378.
Fat intake after breast cancer Lifestyle intervention study 2,437 postmenopausal women with early breast cancer Randomised to nutritional and lifestyle counselling, or not. Eight bi-weekly individual exercise and lifestyle counselling sessions for median 60 months. Results; In the Intervention group: - Dietary fat intake reduction was significantly greater. - Weight was lower - Relapse rate was significantly lower (p=0.03) - Overall survival greater. Chlebowski RT, et al., JCO 2005(10): p. 3s
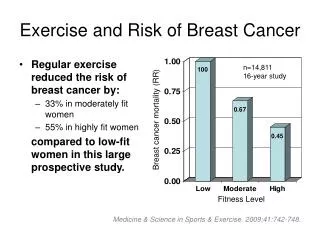
Exercise & Bowel cancer relapse Australian cohort study, 526 patients, colorectal cancer 1990-4,. Exercisers def: recreational sport 1-2 week sweat and breathless Results at 5 yrs - 57% alive (non-exercisers) - 71% alive (exercisers) - statistically significant 14% (p<0.05) - greatest benefit in stage III USA cohort study, 816, colon cancer, stage III. Exercise questionnaire, 18 or more MET-hours of activity a week (6 hours walking at a mod pace) - 35% difference in relapse rate between in the those in the upper to lower quartiles of activity - overall survival significantly different Giles GG, IARC SciPubl, 2002. 156: p. 69-70. Meyerhardt JA, et al., Proc Am Soc ClinOncol, 2005. 24: 3534
Mechanisms - Exercise • Lower IGF-1 and higher IGFBP-3 levels • Serum from exercisers encourage P53 activity • Prostaglandin and COX-2 inhibition • Reduce weight – and help hormonal mileau • Increases the bowel transit time • Reduce cholesterol and lipids
Exercise and breast cancer relapse • 933 BC survivors PE> 2.5 hrs/week 67% reduction in RR (Irwin M et al 2007 JCO) • 4482 BC survivors PE > 2.8 hrs/wk 35-49% reduction in RR (Holick C et al Cancer Epidemiological Biomarkers Prev 2008) • Nurses Health study 2987 BC survivors 3-5 hrs/wk better survival and RR (Holmes et al JAMA 2005) • 1490 BC survivors 30 mins 6 days a wk (+ >5 fruit/veg a day) greater survival (Pierce JP Clin Onc)
Exercise and prostate cancer relapse rates 2,686 men in the Health Professionals follow up study 986-2008 diagnosed with localised prostate cancer 554 died 122 (22%) of prostate cancer. 3 or more MET-hours per week reduced the risk of death by 35% (overall survival) >90mins brisk walking had a 51% reduction in the risk of death 6 or more MET- hours (5 or more hours of vigorous exercise / week e.g. Jogging) had a 56% reduction in the specifical prostate cancer risk of dying. (Kenfield et al 2010)
Cancer Survivorship Exercise Expert Advisory Group Chair: Robert Thomas Manager: Jo Foster
Motivate Educate Research Convince Cost effectiveness Lobby
Local exercise programmesPractical solutions Hospital based programme Hospital based programme Lifestyle counselling & information Community based programme Community based programme Discharge
Activity for Health Referral Scheme • 2001 DoH white paper • Run by PCT who pay for training of instructors • Referral to one of 5,700 municipal leisure centres
80 referrals Pilot evaluation • No adverse events • 44% contacted gyms after initial referral • 38% contacted gyms only after prompting • 10% changed their minds • 82% proceeded to exercise sessions • 100% who started the programme finished (12wks) R Thomas, Pei Ding, M Williams. Is the National activity for health referral scheme the practical solution for exercise rehabilitation after cancer. www.ncri.org.uk/ncriconference/2010abstracts/abstracts/A68.htm
Cancer rehabilitationNational accreditationLevel 4 • Skills active (DoH) • Minimal standards - personal trainers • July 2010 agreed • Course designed April 2011
Evaluation of the cancer exercise rehabilitation programme 400 Patients post initial therapies (Breast, colorectal, prostate) Lifestyle and exercise advice Lifestyle and exercise advice & referral • Primary clinical end points: • Average weekly exercise - The General Practice Physical Activity Questionnaire • Secondary clinical end points: • Qol questionnaire - Psychological Flourishing Scale • Utilisation of health services (laxatives, BP, cholesterol) • Laboratory end points: • Serum IGF levels correlated against exercise levels • Ability of serum from participant to inhibit cancer cell line growth • Cost benefit analysis
More information Lifestyle and cancer – the facts Evidence review for the national survivorship programme cancernet.co.uk/lifetsyle-published-evidence.htm Lifestyle and cancer evidence news summary Sign up: Cancernet.co.uk Email: Health-education@clara.co.uk