Download
1 / 45
450 likes | 798 Views
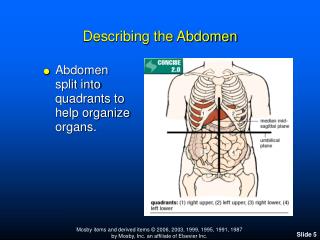
THE PAEDIATRIC ABDOMEN. INTUSSUSCEPTION Diagnosis by Ultrasound Treatment by Imaging and Air Enema. Anne Connell. Mater Children’s Radiology. INTUSSUSCEPTION. PART OF THE INTESTINE FOLDS ON ITSELF LIKE A TELESCOPE. SYMPTOMS Crying Pulling Up Legs Vomiting Stools like “currant jelly”

E N D
THE PAEDIATRIC ABDOMEN INTUSSUSCEPTION Diagnosis by Ultrasound Treatment by Imaging and Air Enema AnneConnell MaterChildren’sRadiology
INTUSSUSCEPTION PART OF THE INTESTINE FOLDS ON ITSELF LIKE A TELESCOPE
SYMPTOMS Crying Pulling Up Legs Vomiting Stools like “currant jelly” PALE
CAUSES 90% Idiopathic Unsure but it is believed that a virus may be the cause.( Anomalies with peristalsis) 10% Pathologic A polyp, tumour or other mass within the intestinal tract is caught by the normal contractions, creating a “lead point” which pushes along causing the intussusception
TYPES of INTUSSUSCEPTION IleoIleal Small bowel/small bowel. May spontaneously resolve Straight to surgery Child with up to 5 at same time.
TYPES of INTUSSUSCEPTION Ileo Cecal Small bowel/ Large bowel Radiology Intervention Air Enema to reduce by “pushing it back”
TYPES of INTUSSUSCEPTION Colocolic Large bowel/large bowel Usually the elderly No Radiology intervention Straight to surgery
Ultrasound examination 1. PRESENCE ? No Full Abdomen scan Yes 2. WHERE IS IT Further down the colon- the longer it’s been there decreases the chance of reduction 3. FLUID Free Fluid and trapped fluid These are signs of possible rupture
4. LEAD POINTS Nodes Polyps Meckel’s Diverticulum Duplication cysts 5.PERFUSSION( Blood Flow) Within the walls of the intussusception Reduced flow can be necrosis BUT oedema also causes this.
AIR ENEMA REDUCTION ENEMA ALWAYS PERFORMED WITH SURGICAL COVER PRESENT AIR REDUCTION ENEMAS ARE ALWAYS ATTEMPTED EASIER THAN SURGERY WITH G.A’s etc.
NECROTISING ENTEROCOLITIS NEC Disease of premature infants in the Intensive Care Unit Breakdown of the mucosal wall of the intestine which allows bacteria &/or air to enter the bowel wall Believed to be related to some combination of infection and ischemia
PRESENTATION First or Second Week of Life SYMPTOMS Abdominal Distension Feeding Intolerance Increased Aspirates From N.G.tube Sepsis
DECUBITUS SUPINE HORIZONTAL BEAM
RADIOGRAPHIC FINDINGS Normal Suggestive Diagnostic
SUGGESTIVE Focal dilation of bowel Featureless “unfolded” appearance of small bowel loops with separation of bowel loops suggestive of bowel wall thickening
N E C Appearance of “unfolding” of loops of small bowel
SUGGESTIVE Focal dilation of bowel Featureless “unfolded” appearance of small bowel loops with separation of bowel loops suggestive of bowel wall thickening An unchanging gas pattern over serial films is of concern.
DIAGNOSTIC Definite Sign PNEUMATOSIS ( gas in bowel wall)
TREATMENT When NEC is suspected Bowel rest ( nothing orally) Antibiotics Monitored with serial abdomen films
DIAGNOSTIC DEFINITE SIGN PNEUMATOSIS ( gas in bowel wall) FREE INTRAPERITONEAL AIR INDICATES SURGERY
anne.connell@mater.org.au Anne Connell
GRATEFUL THANKS FOR ULTASOUND ASSISTANCE Ivan Simic And Dr Umesh Shetty for his advice