Download
1 / 48
510 likes | 879 Views
RESPIRATORY GAS TRANSPORT. Biochemistry Departement Medical Faculty Of Andalas University Padang. Oxygen Transport. Total Body Oxygen Stores . Oxygen in the Lung (~500 ml O 2 ). Oxygen in the Blood (~850 ml O 2 ). Oxygen in the Cells (very little except Mb-bound). At the Lung Level.

E N D
RESPIRATORY GAS TRANSPORT Biochemistry Departement Medical Faculty Of Andalas University Padang
Total Body Oxygen Stores • Oxygen in the Lung (~500 ml O2). • Oxygen in the Blood (~850 ml O2). • Oxygen in the Cells (very little except Mb-bound).
Oxygen Is Carried in Blood in 2 Forms • Bound to hemoglobin in red blood cells. • Dissolved in plasma. Normally insignificant.
Hemoglobin • Each “heme” molecule is capable of binding with 1 O2 molecule and each “globin” molecule is capable of binding with 1 CO2 molecule. • So, each molecule of Hb can bind to either 4 molecules of O2 and 1 molecule of CO2 • 100 ml of blood has about 15 gm of Hb, at Hct = 0.45
Binding of O2 to 4 heme sites given by: • Equilibrium constants for different reactions different • Binding of first O2 relatively low affinity • 2nd, 3rd and 4th - much higher affinity
Oxygen as Oxyhemoglobin • Each gram of Hb can store about 1.34 ml of O2: • 1 L of blood (150 gm of Hb) can store about 208 ml of O2 Oxygen Capacity of Hb. • With normal cardiac output, about 1040 ml of O2 can be carried in blood per minute. (4 times of the metabolic demands).
O2 Saturation. • Units: percent. • Fraction or percentage of all the hemoglobin binding sites that are currently occupied by oxygen.
Four (5-6?) Things Change Oxyhemoglobin Affinity • Hydrogen Ion Concentration, [H+] • Carbon Dioxide Partial Pressure, PCO2 • Temperature • [2,3-DPG] • Special Case: Carbon Monoxide • Hemoglobin variants
Factors Affecting Hb-O2 Affinity: Summary • Hydrogen Ion: • Increased H+ (decreased pH) increases H+ binding to Hb and reduces O2 affinity (HbO2+H+HbH++O2). • Carbon Dioxide (Bohr effect): • Increased PCO2 increases CO2 binding to Hb and reduces O2 affinity (increased O2 delivery to tissue). • Increased PCO2 increases H+ and reduces O2 affinity (fixed acid Bohr effect). • Temperature and 2,3-DPG (diphosphoglycerate): • Increased temperature and 2,3-DPG reduces O2 affinity.
Effect of CO & Anemia on Hb-O2 Affinity Normal blood with Hb=15 gm/dl, anemia with Hb=7.5 gm/dl, and normal blood with 50% HbCO (carboxyhemoglobin).
Exercise • Increase temperature • Increased PCO2 and • Decreased pH (acidosis)
2,3-DPG • 2,3-DPG is a glycolytic intermediate • accumulates to uniquely high levels in RBCs -Increased 2,3-DPG right shift -Decreased 2,3-DPG left shift • Increased 2,3-DPG associated with hypoxia.
Conditions with Increased 2,3-DPG • acclimatization to high altitudes. • chronic lung disease; emphysema. • anemia. • hyperthyroidism. • right to left shunt. • congenital heart disease. • pulmonary vascular disease.
Carbon Dioxide Transport • CO2 is transported in blood in dissolved form, as bicarbonate ions, and as protein-bound carbamino compound. • Protein-bound CO2 (carbamino compounds): • Amount of CO2 stored as carbamino compounds is about 21 ml/L (4% of the total art CO2).
Carbon Dioxide Transport • A majority amount of CO2 is transported in the form of bicarbonate ions (HCO3-): • Amount of CO2 in HCO3- form at PCO2=40 mmHg is about 420 ml/L (90% of the total arterial CO2).
Carbon Dioxide Transport • Haldane Effect: Increasing O2-saturation reduces CO2 content and shifts the CO2 dissociation curve to right. This is because, increasing PO2 leads to : • Decrease in the formation of carbamino compound. • Release of H+ ions from the hemoglobin and resulting in dehydration of HCO3-.
Carbon Dioxide Dissociation Curve Over the normal physiological range (PCO2 = 30 to 55 mmHg and PO2 = 40 to 100 mmHg), the CO2 equilibrium curve is nearly linear. But, O2 equilibrium curve is highly nonlinear.
Bicarbonate in RBCs. • Carbonic anhydrase is present in RBCs • CO2 forms carbonic acid which dissociates to H+ and HCO3- • Released H+ is buffered by histidine residues (imidazole group) • Percent of the total PaCO2: 70%
Carbamino Compounds in RBCs. • Approximately 30% of RBC contents is Hb • CO2 forms carbamino hemoglobin • Released H+ is buffered by histidine residues (imidazole group) • Percent of the total PaCO2: 23 %
CO2Formation in Plasma • Carbamino compounds • CO2 binds the amine groups of plasma proteins to form carbamino compounds.
Chloride Shift (Hamburger Shift) • Newly formed HCO3- passes out of RBC • Cl- diffuses into RBC to maintain electroneutrality • Chloride shift is rapid • Complete before the RBCs exit capillary
Tissue-Gas Exchange: Summary • Gas exchange processes in the peripheral organs are essentially opposite those in the lungs. • O2 is released from the capillary blood to the tissues and diffuses to the mitochondria where O2 is converted to CO2 and energy (ATP) through cellular metabolism. • CO2 diffuses from the tissues to the blood stream and is transported to the lungs for elimination. • The exchange of O2 and CO2 in the blood-tissue exchange unit depends on PO2, PCO2, and also on O2 and CO2 saturation curves.
Pelepasan CO2 • Dilakukan oleh: 1. isositrat dehidrogenase 2. α-ketoglutarat dehidrogenase • Pelepasan CO2 tidak mengkonsumsi oksaloasetat.
Siklus ATP/ADP • Berperan untuk menghubungkan proses-proses yg menghasilkan P-berenergi-tinggi dgn proses yg menggunakan P-berenergi-tinggi. • ATP dikonsumsi & dibentuk kembali secara kontinu. • Depot ATP/ADP sangat kecil, sehingga hanya cukup untuk mempertahankan jaringan aktif dlm waktu beberapa detik saja.
Siklus ATP/ADP ATP CO2 Pernapasan: Penggunaan energi: pembentukan energi - biosintesis makro- dari; - karbohidrat molekul - lemak - kontraksi otot - protein - transpor ion aktif - termogenesis O2 ADP + Pi
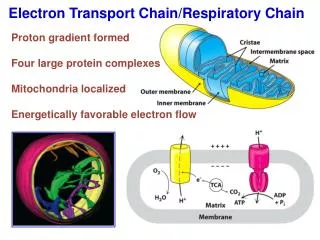
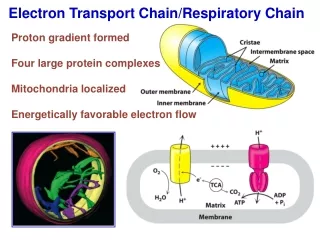
Fosforilasi Oksidatif • Adalah sistem dalam mitokondria yang memasangkan respirasi dengan proses pembentukan intermediat berenergi tinggi, ATP. • Sistem ini memungkinkan organisme aerob menangkap energi bebas dari substrat respiratorik dalam jumlah lebih besar dibanding organisme anaerob.
Peran Rantai Respirasi asam lemak + b-oksidasi gliserol ATP O2 glukosa Asetil KoA SAS 2H H2O rantai respirasi Asam amino ADP mitokondria
Produk ATP pada Fosforilasi Oksidatif Berdasarkan hipotesis kimiosmotik dari Mitchell yaitu; rantai bekerja --> proton dipompa keluar dari membran dlm mitokondria --> pH antar membran turun --> proton balik ke dalam matrik lewat tonjolan ATP-sintase--> fosforilasi ADP menjadi ATP.
Produk ATP pada Fosforilasi Oksidatif • Diperkirakan satu ATP disintesis setiap dua proton melewati tonjolan tsb. • Hasilnya ialah; - 3 mol. ATP utk oksidasi 1 mol. NADH - 2 mol. ATP utk oksidasi 1 mol. FADH2 • Laju fosforilasi oksidatif dikendalikan oleh; NADH, oksigen, ADP
Resources • BIOEN 589: Integrative Physiology. Download 24 jan 05. • Kennelly, PJ., Rodwell, V W. Proteins: Myoglobin & Hemoglobin. In: Harper’s Illustrated Biochemistry. 27th Ed. 41- 8. • Miliefsky, M. Respiratory System Ch.23. Download 24 Nov 10. • Sheardown, H. Blood Biochemistry. McMaster University. Download 20 Mei 07. • Irvin, CG. Respiratory Physiology. Lecture 4A CO2 Transport. In: MEDICAL PHYSIOLOGY 30. Download 22 Jun 09. • Marks, DB., Marks, AD., Smith CM. Basic medical biochemistry: a clinical approach. 1996. Dalam: B.U. Pendit, penerjemah. Biokimia Kedokteran Dasar: Sebuah Pendekatan Klinis. Eds. J. Suyono., V. Sadikin., L.I. Mandera. Jakarta: EGC, 2000 • R.K. Murray, D.K. Granner, P.A. Mayes, V.W. Rodwell Harper’s Biochemistry. 27th ed. McGraw-Hill Companies, New York. 2006.