Download
1 / 46
460 likes | 481 Views
This webinar presentation outlines the types of databases maintained by UNICEF on HIV and AIDS, sources of data, data collection methods, key challenges, data discrepancies, and useful global databases. It covers the Four Ps of UNICEF HIV/AIDS focus areas and the types of data maintained, including indicators on prevention, treatment, HIV prevalence, orphan support, and more. The sources of HIV and AIDS data include nationally representative household surveys like MICS, DHS, and AIS, as well as special behavioral surveys and service provision statistics. The process of joint interagency monitoring of national HIV/AIDS responses is also highlighted, emphasizing coordinated data collection, validation, and reconciliation.

E N D
Overview of Global HIV & AIDS Databases at UNICEF HQ Priscilla Akwara, PhD Senior Adviser, Statistics & Monitoring Section UNICEF, New York Webinar Presentation April 19, 2011
Outline • What type of HIV and AIDS databases are maintained by UNICEF? • What are the sources of data? • How & when are data collected/collated, validated, and up-dated? • Where are the HIV and AIDS data found? • What are the key measurement challenges and sources of data discrepancies? • Other useful global databases on HIV and AIDS • Questions?
UNICEF HIV/AIDS focus areas The Four Ps P1 Prevention of Mother-to-Child Transmission (PMTCT) of HIV P2 Providing Paediatric Treatment of HIV P3 Prevention of Infection among Adolescents and Young People P4 Protection and Support for Children Affected by HIV and AIDS
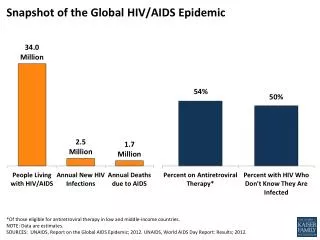
Types of data maintained at UNICEF • Over 70 indicators and estimates on each of the 4 Ps & in line with global goals and targets – MDGs, UNGASS, Universal Access • Indicators • Knowledge of HIV prevention • Misconceptions about HIV and AIDS • Age at sexual debut • Higher-risk sexual partnerships • Condom use during higher-risk sex • HIV prevalence • Orphan school attendance • Care & support for OVC • PMTCT coverage • Paediatric HIV coverage, e.g. ART, cotrimoxazole, testing • Key populations at higher risk • Estimates • Adults & children living with HIV • New HIV Infections • AIDS-related deaths • Treatment needs for ART, PMTCT, cotrimoxazole • Orphans, including AIDS-related
Data disaggregation • Geographic areas • Residence (urban, rural) • Sex • Education • Age • Wealth • Ethnicity/religion • Marital status • Other stratifiers Where possible, indicators can be disaggregated by:
Main sources of data • I) Nationally representative household surveys • Major international survey programmes: • Multiple Indicator Cluster Surveys (MICS) • Demographic and Health Surveys (DHS) • AIDS Indicator Surveys (AIS) • Use standard data collection methodology and questionnairesto allow for country/regional comparisons and trend analysis • Primary sources of disaggregated data • Others include: behavioural surveillance surveys (BSS); Reproductive and Health Surveys (RHS) • Typically, data are collected by countries every 3-5 years
UNICEF support for data collection on women, children and AIDS
The Multiple Indicator Cluster Survey • Household surveys designed to collect data on children and women and to provide evidence base for improved policy formulation and programme planning • Key data source for monitoring the MDGs, the World Fit for Children goals, and other major international commitments • More than 100 indicators (nutrition, child health, mortality, child protection, education, HIV, etc.) • Data available by background characteristics (sex, age, ethnicity, wealth, education, marital status, geographic zones, etc., and/or sub-nationallevels. • Questionnaires, indicators, etc are harmonized with DHS
Multiple Indicator Cluster Surveys (MICS)15 years, 100 countries and 200 surveys Note: Countries with at least one MICS survey.
II. Special Behavioural Surveys • Behavioral surveys among specific sub-populations (e.g. surveys among Injecting drug users, men who have sex with men, or sex workers, donein a specific region(s) in a country) • They provide information on specific sub-populations but cannot be extrapolated to the general population • Mostly implemented every 3-5 years
III. Service provision/programme and surveillance statistics • Coverage statistics are produced by national HIV/AIDS programmes in conjunction with implementing partners– e.g. - Number of HIV positive pregnant women receiving anti- retrovirals to prevent mother-to-child transmission of HIV; Number of children receiving ART • The data provide numerators for calculating indicators on coverage of HIV services - e.g. Percentage of children receiving anti-retroviral therapy • Data for 12-month period (typically Jan-Dec) are requested annually from the Ministries of Health (MoH) or National HIV & AIDS Authorities e.g. National AIDS Commission (NAC) or National AIDS Control Programme (NACP)
Process of joint interagency monitoring of national HIV/AIDS responses • In 2008, WHO/UNICEF/UNAIDS first published one joint report 'Towards Universal Access: Scaling up priority HIV/AIDS interventions in the health sector’ with coordinated data collection and validation • In 2009, UNICEF/WHO/UNAIDS developed the Joint monitoring Form on the health sector response to HIV/AIDS • Annual data are requested from countries through regional offices • Joint memo from head quarters (HQ) of 3 UN agencies to regional and country offices explaining the country reporting process • Globally, joint interagency data validation, reconciliation and harmonization for Universal Access and UNGASS – UNAIDS, UNICEF, WHO, PEPFAR & Global Fund. • Follow up emails to countries to address inconsistent, incomplete, missing or ambiguous data issues • Final data published last quarter of the year • 2011 reporting memo, form, and guidance sent out and data expected at HQ by March 31, 2011.
Joint interagency reports; same programme data • Same data are published in the following joint UN reports: • UNAIDS, Report on the Global AIDS Epidemic, 2010 • WHO, UNICEF, UNAIDS, Towards Universal Access: Scaling up priority HIV/AIDS interventions in the health sector, 2010 • UNICEF, WHO, UNAIDS, UNFPA, UNESCO, Children and AIDS: Fifth Stocktaking Report, 2010
IV. HIV Estimates from statistical Modelling • UNAIDS & WHO in conjunction with UNICEF, CDC, US Census Bureau, and countries organize workshops for generating HIV estimates from statistical models (mainly Spectrum & EPP software) every two years • Regional Estimation workshops for 2010 HIV estimates are ongoing between March - June, 2011. • The estimates are generated based on specific assumptions of national epidemiological and demographic characteristics and programme coverage of HIV services • HIV estimates generated include: • People living with HIV; • New HIV infections • AIDS-related deaths • Treatment needs (e.g. ART, PMTCT, Cotrimoxazole) • AIDS-related orphans • HIV incidence/prevalence
Country Reports on Indicators for the Goals (CRING) • Annual updates of survey data in collaboration with UNICEF country offices • Submissions undergo rigorous review against a set of objective criteria • CRING Online – new process to replace reporting forms • 2011 Deadlines • 31 March/1 April 2011 – COs to be notified • 29 April 2011 – CRING Online closes • May 2011 – HQ contacts COs for any clarifications • Feedback to countries on assessment of results • www.childinfo.org/CRING(password access)
Validating CRING data – accept or reject? (1) Data must meet basic minimum criteria • Does indicator definition/wording match standard definition? • E.g not all 5 components of comprehensive knowledge used to calculate indicator • Higher-risk sex – casual, commercial, non-regular, non-marital, non-cohabiting, multiple sexual partners • Does numerator & denominator match with indicator definition– sometimes different age range from standard definition - e.g. all respondents vs15-24 or 12-25 instead of 15-24 • What is the data source? – e.g. DHS, MICS, AIS, RHS, BSS • Is the survey nationally representative, using a statistically sound sampling approach? • Is sample size adequate for calculation of the indicator?
Validating CRING data – accept or reject? (2) Data must meet basic minimum criteria • Is source documentation specified or provided? • Is the time reference point similar to standard definition – e.g. last 12 months vs 6 months or last 3 months • Do data match those in published report? Sometimes they are transposed or just not found in the report MICS4 Survey Design Workshop
Accessing HIV & AIDS Data • Disaggregated databases are accessible in many UNICEF products and are disseminated widely and available on www.childinfo.org • Disparity databases • Country statistical profiles & fact sheets • Data driven reports • MICS compiler
Inter-agency reports UNICEF flagship reports Country Fact Sheets Sector-specific reports
What are key measurement challenges and sources of data discrepancies?
Key measurement challenges: survey-based indicators (1) • Non-sampling errors that occur because of individual response and socio-cultural biases – affect reliability & validity of data • Discussion of sexual matters is considered taboo in many cultures • Respondent may be exposed to retaliation if privacy and confidentiality is compromised • Sensitive & personal nature of sexual behaviour questions can bias responses - people may report what they believe in and not on expected knowledge • Low response rates and/or small sample sizes • Higher risk sex and condom use among those with higher-risk sex • Orphan school attendance ratio is restricted to double orphans and who are 10–14-year-olds • Retrospective cross-sectional data collection is prone to problems of recall and normative reporting
Key measurement challenges: survey-based indicators (2) • Challenge in finding common terminology for use in data collection – distinction between regular vs non-regular, non-marital, non-cohabiting, and commercial sexual types is often difficult • Common misconceptions about HIV could change over time and affect consistency and comparability of data • The cause of orphanhood is not known so indicator is only proxy of AIDS impact on school attendance
Key measurement challenges: survey-based indicators (3) • Household surveys miss children living in the streets or institutions • Most indicators are more relevant in high HIV prevalence countries than in low and concentrated epidemics • data are not available for most countries, thus affecting calculation of global and regional averages
Potential sources of data discrepancies: survey-based indicators (1) • Use of different wording/definitions • Higher risk sex - casual, commercial, non-regular, non-marital, non-cohabiting, and multiple sexual partners • Not including all 5 components of comprehensive knowledge • Single orphans (only mother or father dead) vs double orphans (both parents dead) • Use of school attendance in the last year instead of current school attendance • Use of different reference time points - specific time durations have not been uniform (last three, six or 12 months) – affects calculation of comparable indicators and trends • Use of different sources of data, e.g. national vs sub-national or targetted surveys vs service statistics vs estimates of coverage
Potential sources of data discrepancies: survey-based indicators (2) • Use of different denominators: • - all respondents vs only sub-populations • - all ages or different age bands (10-24 or 12- 15years) vs 15-24 year olds • - for orphan school attendance – 0-17 or 0-14 vs 10-14 year olds
Key measurement challenges : programme data and estimates (1) • Poor programme data quality due to weak national monitoring systems: • Inconsistencies e.g. disaggregation totals not adding up; reported numbers far lower or higher than for previous reporting period • Incomplete data - reporting period missing; reporting period less than one year, or report from only a sub-set of facilities • Often, data from private facilities excluded – not a comprehensive reflection of country programme performance • Timeliness – data not reported on time or never reported • Double or triple counting is common • Parallel M&E systems hence multiple data received for the same reporting period through different departments of government HMIS, NACs or NACPs
Key measurement challenges: programme data and estimates (2) • Trend analysis for coverage is challenging since data sources are different – routine programme data (numerator) and statistical modelled estimates (denominator); • Proportion of people needing HIV services can change rapidly e.g. ART, PMTCT vary with the stage of the HIV epidemic and the effectiveness of the treatment regimens among adults and children, including with changes in treatment guidelines • Coverage is based mainly on data from low- and middle-income countries only – regional and global averages are limited to these countries • Lack of disaggregated data; OR disaggregated data do not add up to the reported total
Potential sources of data discrepancies: programme data and estimates (1) • Different indicator definitions – e.g. • Adults/children currently on ART vs cumulative number of adults/children ever started on ART which does not account for patients who have died, stopped treatment or lost to follow-up • Variations in the methodology of calculating estimates of people in need of HIV services and coverage at global & national levels • International agencies generate national estimates using a standard methodology while countries may use only registered cases thus underestimating need for services and overestimating coverage
Potential sources of data discrepancies: programme data and estimates (2) • Use of adjustment factors for double counting and undercounting – international agencies use; while most countries do not • Use of weighted averages for calculating regional and global estimates at global, while most regions do not • Estimates of need & coverage are recalculated retrospectively each time the estimation methodology is revised, while countries might continue to use old estimates • Countries may use most recent updated data once final counts are in, whereas global agencies use most recently validated and published annual aggregate national data
Other useful databases • UNAIDS AIDSinfo- http://www.unaids.org/en/dataanalysis/tools/aidsinfo/ • HIV/AIDS Survey Indicators Database – http://www.measuredhs.com/hivdata/ • MDG database - http://mdgs.un.org/unsd/mdg/Data.aspx • HIV and AIDS Data Hub for East Asia & Pacific and South Asia - http://www.aidsdatahub.org/ • The global AIDS report 2010 - http://wwwunaids.org/globalreport/Global_report.htm • All the narrative reports submitted by countries - http://www.unaids.org/en/dataanalysis/monitoringcountryprogress/2010progressreportssubmittedbycountries/ • National AIDS Spending Assessment (NASA) country reports http://www.unaids.org/en/dataanalysis/monitoringcountryprogress/nasacountryreports/ • Key Monitoring and Evaluation guidance and tools - http://www.unaids.org/en/dataanalysis/tools/monitoringandevaluationguidanceandtools/ Note: These databases are not maintained by UNICEF and might use different data inclusion criteria
Questions? THANK YOU