Download
1 / 49
671 likes | 1.6k Views
Management of TMJ disorders. Part1. Introduction-TMJ. Joints Anatomy Developmental Anatomy Classification Functional/Surgical Anatomy. TMJ Development. The mandible and TMJ develop from the first pharyngeal arch both are innervated by the fifth cranial nerve

E N D
Introduction-TMJ • Joints • Anatomy • Developmental Anatomy • Classification • Functional/Surgical Anatomy
TMJ Development • The mandible and TMJ • develop from the first pharyngeal arch • both are innervated by the fifth cranial nerve • (providing both sensory and motor innervation) • By the 6th week of human gestation • Meckel’s cartilage (primary cartilage) extends from the developing ear to approximately the midline
TMJ Development • By the 9th week of human gestation • The rudimentary mandible is formed by “intramembranous ossification”
TMJ Classification • Anatomic Classification: • Diarthrodial= literally means two articulations • a joint that contains the following characteristics • a freely movable joint ( Discontinuous articulation of two bones • bony surfaces are covered with hyaline or fibrocartilage • lined by a synovial lining and contains synovial fluid • Ginglymoid –Joint has hinge like movement component
TMJ Classification • Functional classification: • Compound joint: A joint composed of three or more skeletal elements • Ginglymoarthroidal Joint • Ginglymoid joint that allows hinge like motion (inferior joint space) • Arthroidial joint that allows translator or gliding movement (superior joint space)
TMJ Classification • The mandible functions as a class III lever system • Load is occlusal surface • Fulcrum is formed by TMJ joint • Force is from muscles of mastication
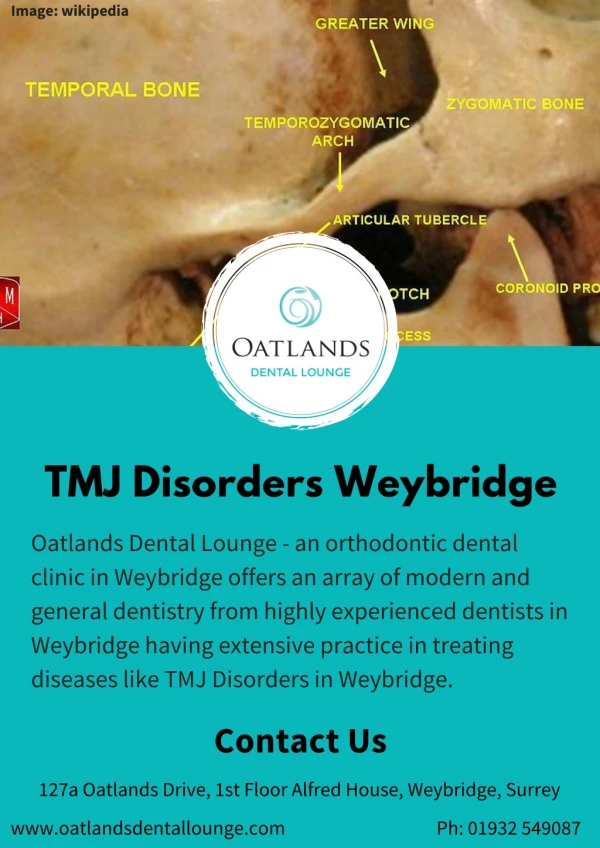
6 components of TMJ • Osseous Components • Condyles • Articular surface of temporal bone • Soft tissue components • Capsule • Articular Disc • Ligaments • Muscle-Lateral Pterygoid
Bony Anatomy • The articular portion of the temporal bone consists of 3 parts: • GlenoidFossa (aka Mandibularfossa) • Articular eminence • Preglenoid plain
Bony Anatomy • Glenoidfossa • Contains lateral and medial rims • Roof of the fossa is thin and separates the brain from the joint cavity • The articular surfaces of the temporal and condylar bones are covered by Fibrocartilage
Bony Anatomy • Fibrocartilage: • Contains a greater proportion of collagen fibers than hyaline cartilage • has a significant capacity to regenerate and to remodel • Contains few blood vessels • primarily nourished by diffusion
Bony Anatomy • Condyle • Condylar Heads (Paired) • 145-160º angle to each other • Covered by fibrocartilage • Individual Condylar Head • 15-20 mm in diameter • 8-10 mm in A-P dimension • Medial and lateral tubercles provide attachment to the collateral ligaments
Articular Disc • Articular Disc • Dense fibrous connective tissue • Devoid of any blood vessels or nerve fibers(extreme periphery is mildly innervated) • Sagittal Plane • Anterior Band • Posterior Band • Intermediate zone
Articular Disc • During function-Adapts to functional demands • Attachments • Posterior attachment- RetroDiscal tissue • Superiorly- Superior retroDiscal lamina • Inferiorly-Inferior retroDiscal lamina
Articular Disc • The articular Disc • divides the joint into a superior and inferior joint space • Joint space volumes • Classically, • Superior space = volume 1.2 ml • Inferior space = volume 0.9 ml • However, recent arthroscopic studies have suggested • Superior space=0.5 ml • Inferior space = 0.3 ml • This helps to stabilize the Disc during function
Articular Disc • Anterior Attachment • Capsular ligament forms-Superior and Inferior attachments-
RetroDiscal Tissue • RetroDiscal Tissue • “the bilaminar zone” • Highly vascular • Highly innervated tissue • superior retroDiscal lamina • inferior retroDiscal lamina
RetroDiscal Tissue • “superior retroDiscal lamina” • superior aspect of the retroDiscal tissue • Contains elastic fibers • Attaches to the tympanic plate • “inferior retroDiscal lamina” • the inferior aspect of the retroDiscal tissue • Consists of collagen fibers without elastic tissue • Attaches to the posterior margins of the condyle
Anterior region • Superior attachment • Anterior margin of articular surface of temporal bone • Inferior Attachment • Anterior margin of the articular surface of the condyle
Ligaments • 3 primary ligaments: • Collateral ligaments • TMJ capsule • Temporomandibular ligament
Ligaments • Accessory ligaments: • Sphenomandibular ligament • Stylomandibular
TMJ Innervation • Sensory innervation • Primarily from the auriculotemporal nerve (the mandibular branch of the trigeminal nerve) • Other contributing nerves • Masseteric nerve • Deep temporal nerve • Motor innervation to the muscles of mastication • Mandibular branch of the trigeminal nerve
Case Presentation • CC: 26 years ♀ presents to the OMS clinic with complaint of • left jaw pain • Intermittent right jaw popping and • inability to open her mouth completely • HPI: • Patient volunteers the following information: • Pt reports a h/o intermittent bilateral jaw joint popping and clicking since she was 16 • Approximately 2 years ago her left jaw quit popping and began to hurt more • Since that time her left jaw joint pain has progressively increased • When asked where it hurts she points to her left TMJ area
Examination of TMJ • Interview • Examination of Masticatory system • TMJ examination • Digital Palpation • Mandible is stationary • Dynamic movement • Check for Pain and tenderness • Sounds • Restrictions
Digital Palpation • Method-step1 • Simultaneously place fingers on both joint areas • Ask the patient to open and close a few times for confirmation • Lateral poles are palpated passing downwards and forward across the articular eminence • Apply medial force and patient to report any symptoms • Record pain on a scale of 1-10
Digital Palpation-Step2 • Ask the patient to open his/her mouth • Rotate the fingers posteriorly • apply gentle force to the posterior aspect • Helps in evaluating any posterior capsulitis or retroDiscitis • Record the areas of tenderness and which part of the opening and closing cycle is it experienced
Sounds • Clicking-distinct sound • Crepitation- scraping or grating sound • Usually associated with Osteoartheritis • Changes in articular surfaces of joint • Louder sounds (sometimes referred to as ‘POP’)
Joint Restrictions • Normal range of motion-straight and symmetric • Interincisal-45mm • Protrusive -10mm • Lateral-10mm • Types- • Extracapsular • Intracapsular
Radiographic Evaluation • Panoramic • Bony anatomy, overall architecture of joint • Tomograms • TMJ Arthrography (Injecting contrast material) • Allows intra-articular Disc visualization • Presence of perforations adhesions
Radiographic Evaluation-contd. • Computed Tomography • Hard and soft tissue morphology • Most accurate assessment of Bony components • MRI • Best for soft tissue elements of TMJ • Dynamic join functions are visualized • Advantage-No ionizing radiation is used • Nuclear Imaging • IV injection of technetium99( Gamma emitting Isotope)
Classification of TMJ disorders • MPD • Disc Displacement • Degenerative Joint disease • Systemic Arthritic Conditions • Chronic recurrent dislocation • Ankylosis • Intrcapsular /Extracapsular • Neoplasia • Infections
Myofacial Pain Dysfunction • Most common cause of Masticatory Pain • Source-Muscular • Muscles of mastication –tender • Abnormal muscle function • Hyperactivity • Clenching or Nocturnal Bruxism • Etiology- Multifactorial ( bruxism,stress, Anxiety, faulty occlusion)
Myofacial Pain Dysfunction • C/F: • Diffuse pain in preauricular area • May involve muscles of mastication • Nocturnal Bruxism • Pain is increased iin the morning • Decreased jaw opening while chewing • Bitemporal headaches • TMJ’s are non tender on palpation • Range of mandibular movement is reduced • Wear facets on teeth
Disc Displacement Disorders(Internal derangement) Anterior Disc displacement with reduction Anterior Disc displacement without reduction
Wilkes Classification • Early Stage • Stage 1 • Mild Disc displacement with normal Disc morphology • Reduction relative to condyle with mouth opening • Intermediate stage • Stage 2 • Mild to moderate Disc displacement and deformity • Reduction with opening • Stage 3 • Disc displacement, deformity and non reduction of Disc with opening • Responds best to surgery • Late stage • Stage 4 • Severe displacement, deformity, shortening or rarely elongation • Non reduction of Disc • Stage 5 • Perforation of Disc attachements • Severe derangement of joint • Regressive remodeling/ osteoartheritis
Anterior Disc displacement with reduction • Disc position • Mouth closed -anterior and medial to condyle • Opening- condyle moves over posterior band of Disc and then returns to normal condyle Disc relationship(i.e. resting on intermediate zone) • Closing-condyle slips posteriorly , rests on retroDiscal tissue, Disc returns to anterior and medial displaced position
Anterior Disc displacement with reduction • Clinical features • Joint tenderness • Clicking –during opening • a closing click (reciprocal click)can also be elicited • MRI best demonstrates
Anterior Disc displacement without reduction • Condyle does not translate anteriorly to its full extent • No clicking (lack of translation of condyle over posterior aspect of the Disc) • Limitation of mouth opening • Deviation of mandible to affected side • Decreased lateral excursions to contra lateral side
Degenerative Joint Disease(DJD) • Anatomic findings- • Irregularities in Disc • Perforations Severely damaged Discs • Clinical features • Pain associated with Clicking • Limitation in mouth opening • Radiographic features • Surface erosions • Decreased joint space • Flattening of condylar head • Irregularities in Mb fossa and articular eminence
Systemic Arthritic conditions(SAC) • Rheumatoid arthritis • Inflammatory process • Radiographic Features- • Erosive changes in anterior and posterior condylar head • Differences between DJD and SAC( RA, lupus) • RA-bilateral joint involvement • RA-Earlier onset than DJD
Subluxation • Hyper mobility • Cause- • Anatomy-short posterior slope articular eminence followed by a longer ,flatter anterior slope • Spontaneous Dislocation • Mouth is opened beyond its normal limit • Mandible locks • Patient cannot close the mouth
Ankylosis • Intracapsular • Fusion of condyle, Disc, Fossa Complex • Partial reduction to complete immobility • Etiology-Trauma***,Previous surgical treatment, Rarely infections (otitis media) • C/F-Resticted Jaw opening • Deviation to affected side • Fibrous Ankylosis-jaw opening is present • Bony Ankylosis- No movement • Extracapsular • Condylar hyperplasia • Enlarged cornoid process