Download
1 / 10
100 likes | 291 Views
Diagnosis of Metabolic disorder process . Metabolic acidosis . Secondary Ventilatory Response

E N D
Metabolic acidosis • Secondary Ventilatory Response • When the metabolic acidosis is prolonged for approximately 24h or longer, the expected PaCO2 for any value of stable serum HCO3- concentration can be derived using the following formula, familiarly referred to as Winter's formula: PaCO2 = 1.5[HCO3-] + 8 ± 2 • Other studies have indicated that the appropriate Δ PaCO2 can be calculated by multiplying the Δ HCO3-concentration by 1.2.
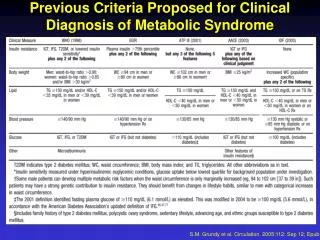
Serum Anion Gap • The serum anion gap, defined as [Na+] - ([Cl-] + [HCO3-]), is a valuable diagnostic tool as the various disorders that produce metabolic acidosis can affect the serum anion gap differently. • No change in the anion gap is observed in some disorders (normal anion gap or hyperchloremic acidosis), whereas in other disorders the serum anion gap is increased (high anion gap metabolic acidosis). Mixed normal and high anion gap patterns are also common. • The normal range for the serum anion gap is relatively wide (6-10 mmol/l), a finding that reflects the biologic variability of its constituents. In addition, mean values from different clinical laboratories vary: mean serum anion gap was 11 ± 2.5 mmol/l in one laboratory and 6 ± 3 mmol/l in another. • Lower mean values result from the higher serum Cl-concentration obtained when using an ion-specific electrode. • Knowledge of the mean and range of normal values for the serum anion gap for a particular laboratory and the baseline value of an individual's anion gap are therefore necessary for optimal interpretation of a change in value.
Metabolic alkalosis • If the urinary Cl is low, indicating a hypovolemic state, then administration of NaCl and water to replenish the extracellular volume should stop the stimulus for aldosterone production and in turn should lead to appropriate excretion of excess HCO3- and improvement of hypokalemia. • Thus, leading to correction of the metabolic alkalosis. Such causes of metabolic alkalosis are said to be saline responsive.
Metabolic alkalosis cont’d • Metabolic alkalosis also diagnosed by measuring serum electrolytes and arterial blood gases. • If the etiology of metabolic alkalosis is not clear from the clinical history and physical examination, including drug use and the presence of hypertension, then a urine chloride ion concentration can be obtained. • Calculation of the serum anion gap may also help to differentiate between primary metabolic alkalosis and metabolic compensation for respiratory acidosis.
LABORATORY TEST FOR METABOLIC ACIDOSIS AND ALKALOSIS • The primary tests used to identify, evaluate, and monitor acid-base disorders are: 1. Blood gases 2.Electrolytes
Blood Gases • Blood gases are a group of tests performed together, usually on an arterial blood sample where blood obtained from an artery instead of a vein. They are a snapshot of the blood's pH, PO2 (the amount of oxygen in the blood), and PCO2 (the amount of carbon dioxide the blood). • From these results, bicarbonate (HCO3-) can be calculated. In most acid-base disorders, both HCO3- and PCO2 are outside the reference range. That is because the body tries to keep the pH close to normal. Therefore, if one of these substances is abnormally high or low, the other one will change in the same direction to bring the pH back toward its healthy range. • This process is called compensation. The table below shows the expected values for each of the four main acid-base disorders.
Electrolytes • Electrolytes refers to a group of four tests: Na+ (sodium), K+ (potassium), Cl- (chloride), and bicarbonate that usually measured as total CO2 content. • Body fluid levels, electrolyte concentrations, and acid-base balance are interconnected. • One or more of the electrolytes is usually increased or decreased in metabolic acid-base disorders. In patients with a metabolic acidosis, the anion gap is calculated using the results of an electrolyte panel to help determine which disorders might be responsible for the acid-base abnormality. • For example, an increase in the anion gap can indicate diabetic acidosis.
Electrolytes cont’d • HCO3-Normal : 22 – 26 mEq/LMetabolic Acidosis : < 22 mEq/LMetabolic Alkalosis : > 26 mEq/L