Download
1 / 23
280 likes | 1.01k Views
Pathomechanics of Knee Joint (part 1) practical section. Lecturer: Dr. Manal Radwan Salim Demonstrators: Dr.Mohammed Arafaat Dr. Haytham Essawy Dr. Atef Mohammed Dr. Mai Tolba 3 rd practical section Fall 2013-2014 20-10-2013. Knee/ Leg Anatomy. Arthrology and Movements

E N D
Pathomechanics of Knee Joint (part 1) practical section Lecturer: Dr. ManalRadwanSalim Demonstrators: Dr.MohammedArafaat Dr. HaythamEssawy Dr. Atef Mohammed Dr. Mai Tolba 3rd practical section Fall 2013-2014 20-10-2013
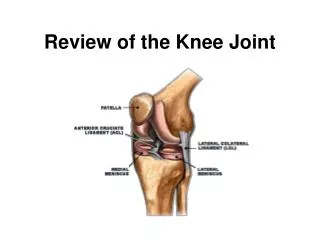
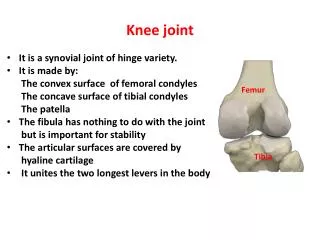
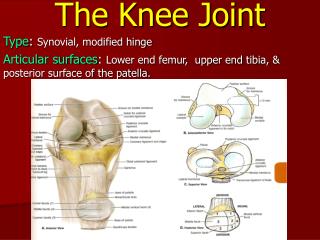
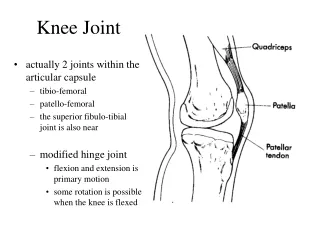
Knee/ Leg Anatomy Arthrology and Movements • Lateral and medial tibiofemoral: • Consist of articulation between large convex femoral condyles, and nearly flat and smaller tibial condyles. • b) Patellofemoral: • Knee stability depends mainly on soft tissue constraints rather than bony configuration.
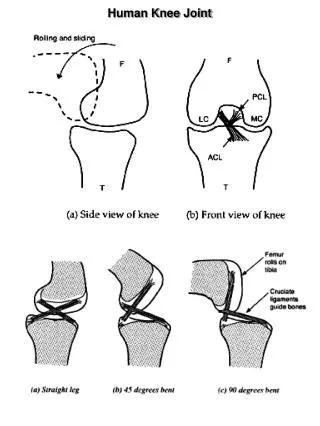
Tibio-fermoral joint flexion / extension movements: occur about medio-lateral axis of rotation. In general a healthy knee rotates from 130-to 140 degrees of about 5 to 10 degrees of hyperextension. The mediolateral axis or rotation is not a fixed point by migrates within the femoral condyles, as it is influenced by the ecentric configuration of the femoral condyles.
*Active extension of the knee: During tibial on femoral extension “open kinematics chain”: The articular surface of the tibia rolls and slides anteriorly on the femoral condyles. The meniscus are shown to be pulled anteriorly by quadriceps muscle. The importance of the sliding movements of tibia and femur during active flexion and extesnion (rolling) is that it allow allow the larger diameter of the spherical femoral condyles to roll over a much smaller transverse surface of the tibial plataeu.
b) During femoral on tibial extension “closed kinematics chain: as in standing up from a deep squat position, the femoral condyles simultaneously roll anteriorly and slide posteriorly on the articular surface of the tibia.
*Active flexion of the knee: a) During tibial on femoral flexion “open kinematics chain”: The articular surface of the tibia rolls and slides posteriorly on the femoral condyles. The meniscus are shown to be pulled posteriorly by popliteus muscle.
b) During femoral on tibial flexion “closed kinematics chain: as in moving from erect standing to deep squat position, the femoral condyles simultaneously roll posteriorly and slide anteriorly on the articular surface of the tibia.
Tibio-fermoral joint internal / external rotation movements: *Internal / external rotation movements occur about vertical or longitudinal axis of rotation. *Rotation degree of knee increases with greater knee flexion. A knee flexed 90 degrees permits about 40 -50 degrees of total rotation, with external rotation range exceeds rotation of internal rotation by a ration 2:1 *In full extension, no rotation is allowed in fully extended knee. *Rotation occur either by tibial rotation on femur in open kinematic chain activities, or femur rotating on tibia in a closed kinematic chain activities.
Generally speaking to all rotating joints (hip, shoulder, knee) the rotation direction (internal or external) is named according to direction of movement of the distal bony segment of the joint; for example knee rotation is named according to movement direction of tibia even if the moving part is the femur in closed kinematic chain. • *In Tibiofemoral rotation (open kinematic chain): • In internal rotation: • the tibia internally rotate, foot moves to points medially. • In external rotation: • the tibia externally rotates, foot moves to point laterally.
*In Femorotibial rotation • (Closed kinematic chain) : • In internal rotation: • The femur externally rotate, foot fixed on ground in neutral the head of femur moves (forward) anteriorly in transverse plane. • In external rotation: • The femur internally rotate, foot fixed on ground in neutral the head of femur moves backward (posteriorly) in transverse plane.
Screw home “rotation of the knee • Locking knee on full extension requires knee rotation about 10 degrees. • Screw home rotation is different from axial rotation that occur at knee it is a conjunct rotation, linked mechanically to flexion and extension kinematics and cant be performed independently. Based on observable twisting of knee during last 30 degrees of extension. • *In tibiofemoral extension: the tibia externally rotates about 10 degrees. • *In femorotibial extension (rising from squat): The femur internally rotates on fixed tibia. • *Regardless whether tibia or femur is rotating the knee is externally rotated 10 degrees when fully extended.
To observe the screw home mechanism: at the knee, have the partner sit with the knee flexed to about 90 degrees. Draw a line on the skin between the tibial tuberosity and the apex of the patella. After completing full tibial –on femoral extension, redraw this line between the same landmarks and note the change in position of the externally rotated tibia.
Unlocking mechanism to unlock the knee that is fully extended, the joint must first internally rotate by poplitues muscle that is both internal rotator and flexor of the knee joint, the muscle can rotate femur externally to initiate femoral-on tibial. flexion, or rotate the tibia internally to initiate tibial –on- femoral flexion. As the extended and locked knee prepares to flex (e.g. when beginning to descend into a squat position), the popliteus provides an internal rotation torque that help mechanically to unlock the knee. In this position the femur is externally rotated on tibia , this action on femur is readily seen by this figure showing line of pull of popliteus
Factors guiding screw home mechanism 1- shape of medial femoral condyle: as it curves 30 degree laterally as it approaches the intercondylar grove. And as and extends further anteriorly than the lateral condyle. Thus tibia must follow this path during tibial on femoral extension. 2- passive tension in the anterior cruciate ligament 3- lateral pull of quadriceps tendon.
Knee joint alignment as in x ray : Femoral mechanical axis:- centre of femoral head to centre knee. b) Femoral anatomical axis”: - centre of femoral shaft to center of knee joint. 6ooutwards from mechanical axis. c) Tibial mechanical / anatomical axis:- centre plateau to centre of talus / ankle
Assessment of joint alignment using motion analysis: 1- identify bony land marks that marks the beginning and ends of each bony segments (forming the tested joint and marks them by colored markers. 2-Fotograph patient in the desired functional position with marks on bony segments ends. 3- Using AutoCAD program draw a straight line that connect between bony segment ends marks. This line represents the mechanical or anatomical axis of the bony segment . 4- Measure the angle between the two drawn anatomical axes.
How to assess knee joint alignment in frontal plane 1- Identify bony land marks: a) Femoral mechanical axis: from centre of femoral head ( 3 fingers medial to ASIS)to centre knee(mid point between medial and lateral femoral epicondyles). Or b) Femoral anatomical axis”: - centre of femoral shaft (at same level as greater trochanter move anteriorly cneter of thigh) to centre knee joint (as above). c) Tibial mechanical/anatomical axis (same): from center of knee (mid point between medial and lateral femoral epicondyles) to center of ankle joint (mid point between lateral and medial maleolus.
How to assess knee joint alignment in frontal plane cont. 2-Fotograph patient in the anatomical position in frontal view. 3- Using AutoCAD program draw mechanical axis or anatomical axis of femur, mechanical (anatomical ) axis of tibia. 4- Measure the outer angle between the two drawn axes. From the above we understand that the exact value of varus or valgus of knee depends on method of measurement whether measuring by anatomical axis or mechanical axis.
Normal genuvalgum: normal alignment is distal end of femur makes an angle of 170 -175 with the anatomical axis. note an angle of 170-175 degree equals 5-10 degrees valgus Note that if measuring from mechanical axis the measured angle will increase to the same person, i.e. normal valgus degree is less? Some authors reported that it is 182 degree, i.e. 2 degrees of varus
A) Excessive Genuvalgum(knock knees): the measured angle lateral is less than 165 degree. i.e. genuvalgus degree is >15 degree Notes: 1- the feet are separated from each others more than knees. 2- the angle opens laterally
B) Genuvarum (bow leg): the measured angle lateral is more than 185 degree. i.e. genuvarum degree is >5 degree Notes 1-the feet are nearer to each others than knee. 2-in varus the angle opens medially
How to assess knee joint alignment in sagitalplane 1- Identify bony land marks: Femoral anatomical (mechanical) axis: from greater trochanter to knee to lateral femoral epicondyle. Tibial anatomical (mechanical) axis: from lateral femoral epicondyle to lateral maleoulus. 2-Fotograph patient in the anatomical position in sagital view. 3- Using AutoCAD program draw femur and tibia bones axes 4- Measure the front angle between the two drawn axes.
Genurecarvatum the measured angle frontal is more than 190 degree. i.e. genurecarvatum (hyperextension)degree is >10 degree Notes 1-the knee are leveled beyond the ankle joint