Download
1 / 39
390 likes | 510 Views
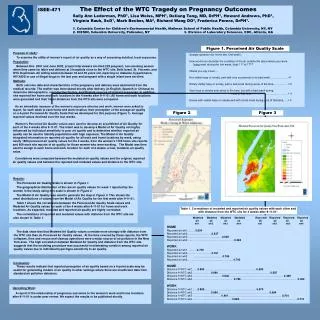
the intersection of the Ryan WHITE HIV/AIDS Program WITH THE essential health benefits in Private Health Insurance AND MEDICAID. HIV/AIDS Bureau, Health Resources & Services Administration; Center for Medicaid and CHIP Services; Center for Consumer Information and Insurance Oversight.

E N D
the intersection of the Ryan WHITE HIV/AIDS Program WITH THE essential health benefits in Private Health Insurance AND MEDICAID HIV/AIDS Bureau, Health Resources & Services Administration; Center for Medicaid and CHIP Services; Center for Consumer Information and Insurance Oversight
Purpose of Webinar • Educate Ryan White grantees about potential new coverage options and the essential health benefits available to PLWH through Medicaid and the Health Insurance Marketplace • Review individual and small group commercial plan coverage of essential health benefits inside and outside of the Health Insurance Marketplace • CMS – Center for Consumer Information and Insurance Oversight (CCIIO) • Review Medicaid coverage of essential health benefits • CMS - Center for Medicaid and CHIP Services (CMCS) • Review how essential health benefits offered in Medicaid and the Marketplace intersect with the Ryan White HIV/AIDS Program • HRSA – HIV/AIDS Bureau & Office of Policy Analysis and Evaluation
Health Coverage Options for PLWH BEFORE the Affordable Care Act Note: Data only reflective of Ryan White clients, not of entire HIV/AIDS population; Source: 2010 Preliminary Ryan White Services Report Data (RSR)
Health Coverage Options for PLWH AFTER the Affordable Care Act Employer-Based Insurance Health Insurance Marketplace Other Private Other Public Ryan White Program PLWH eligible for health coverage Cover comprehensive HIV medical and support services not covered, or partially covered, by public programs or private insurance Cover comprehensive HIV medical and support services not covered, or partially covered, by public programs or private insurance PLWH who remain uninsured
Private Health Plans & Essential Health Benefits Allison Wiley, Health Insurance Specialist Lisa Cuozzo, Health Insurance Specialist Helaine I. Fingold, Health Insurance Specialist Center for Consumer Information and Insurance Oversight (CCIIO)
Introduction • Under the Affordable Care Act: Non-grandfathered health plans offered in the individual and small group markets (inside and outside of the Exchanges) must cover the essential health benefits package, which includes: • Coverage of at least 10 categories of benefits and services (EHB) • Meeting certain actuarial value (AV) standards • Meeting certain limits on cost sharing
Background on Essential Health Benefits The ACA states that EHB must cover at least the following 10 categories of benefits & services: 1. Ambulatory Patient Services 2. Emergency Services 3. Hospitalization 4. Maternity and Newborn Care 5. Mental Health and Substance Use Disorder Services, Including Behavioral Health Treatment 6. Prescription Drugs 7. Rehabilitative and Habilitative Services and Devices 8. Laboratory Services 9. Preventive and Wellness Services and Chronic Disease Management 10. Pediatric Services Including Oral and Vision Care
Benchmark Plan Approach for Essential Health Benefits • Essential Health Benefits are based on a benchmark plan selected by each state • Benchmark options include plans typically offered by small employers • Preserves state flexibility • Similar to the benchmark approach currently used in other programs • Benchmark plans were selected in March 2012, but must conform to all ACA requirements in 2014
Supplementing the State Base-Benchmark Plan to State’s EHB-Benchmark Plan • The Benchmark plan serves as a reference plan: • EHB plan benefits must be “substantially equal” to the benchmark’s benefits • Benchmark plans must cover all 10 statutory categories • A base-benchmark plan that lacks a statutory category must supplement the entire category from another benchmark plan option • A number of states’ base-benchmark plans did not include coverage of pediatric oral & vision care • The final rule allows the state’s base-benchmark plan to be supplemented with: • The FEDVIP pediatric vision/dental plan; or • The state’s separate CHIP plan benefit, if one exists
Supplementing Options for Habilitative Services • A number of state benchmark plans did not include habilitative services • If a state’s benchmark plan does not include coverage of habilitative services, the State may determine which services are included • If a state’s benchmark plan does not include coverage of habilitative services and the State did not define, insurers must: • Provide parity by covering habilitative services benefits that are similar in scope, amount, and duration to benefits covered for rehabilitative services; or • Decide what services to cover & report to HHS
EHB Prescription Drug Benefit • Plans must cover at least the greater of: • One drug in every USP category & class; or • The same number of drugs in each USP category & class as the EHB-benchmark plan • Requires an exceptions procedure so enrollee can gain access to drug not on the plan’s list • Applies discrimination protections • Requires plans to report drug lists to the Exchange, state, or OPM
Requirements for Mental Health and Substance Abuse Benefits • Plans must comply with parity standards for the mental health & substance use disorder services • Based on requirements in Mental Health Parity and Addiction Equity Act of 2008 • EHB rule extended parity to small group plans
Consumer Resource: Actuarial Value • AV standards will help consumers compare health plans by providing information about relative plan generosity • (Total Overall Health Costs – Total Enrollee Cost Sharing)/Total Overall Health Costs • AV must be calculated based on the provision of EHB to a standard population • AV is reflected as a percentage
AV Levels of Coverage • AV determines a health plan’s metal level tier • ACA - directs that non-grandfathered individual & small group plans inside & outside the Exchanges meet particular AV targets (or be a catastrophic plan1): • Bronze = 60% AV • Silver = 70% AV • Gold = 80% AV • Platinum = 90% AV 1Catastrophic plans are only available for certain eligible individuals
Consumer Protections: Non-Discrimination Standards • The EHB rule prohibits discrimination in benefit design based on: • Age • Expected length of life • Disability • Medical dependency • Quality of life • Other health conditions • Allows for reasonable medical management techniques
Consumer Protections: Cost-Sharing • On or after January 1, 2014: • Provides annual limits on maximum out-of-pocket (MOOP) for all group health plans (including large and self-insured): • $6,350 for self-only coverage; or • $12,700 for other than self only coverage • Provides deductible limits for small group market: • $2,000 for self-only coverage • $4,000 for other than self-only coverage • For subsequent plan years: • Will increase based on a premium adjustment % • Applies to in-network costs
Medicaid Alternative Benefit Plans and Essential Health Benefits Melissa Harris, Division Director Christine Hinds, Technical Director, Division of Pharmacy Centers for Medicaid and Chip Services (CMCS)
Background • Intended to be an alternative benefit plan to the Medicaid state plan • Comparability and statewideness are waivable • States define populations, benefit packages and identify delivery systems within SPA • Cost sharing and payment methodology SPAs required if applicable • May require changes to other authorities such as 1115s or 1915(b) waivers
Final Regulation Overview • Section 1937 Medicaid Benchmark or Benchmark Equivalent Plans are now called Alternative Benefit Plans (ABPs) • ABPs must cover the 10 Essential Health Benefits (EHB) as described in section 1302(b) of the Affordable Care Act, whether the state uses an ABP for Medicaid expansion or coverage of any other groups of individuals • Individuals in the new adult eligibility group will receive benefits through an ABP
Ten Essential Health Benefits 1. Ambulatory Patient Services 2. Emergency Services 3. Hospitalization 4. Maternity and Newborn Care 5. Mental Health and Substance Use Disorder Services Including Behavioral Health Treatment 6. Prescription Drugs 7. Rehabilitative and Habilitative Services and Devices 8. Laboratory Services 9. Preventive and Wellness Services and Chronic Disease Management 10. Pediatric Services Including Oral and Vision Care
Steps for Designing a Medicaid ABP • Step 1: States must select a coverage option from the choices found in section 1937 of the Act • Four benchmark options • (1) The Standard Blue Cross/Blue Shield Preferred Provider Option offered through the Federal Employees Health Benefit program • (2) State employee coverage that is offered and generally available to state employees • (3) Commercial HMO with the largest insured commercial, non-Medicaid enrollment in the state • (4) Secretary-approved coverage, a benefit package the Secretary has determined to provide coverage appropriate to meet the needs of the population
Steps for Designing a Medicaid ABP (continued) • Step 2: States must determine if that coverage option is also one of the base-benchmark plan options identified by the Secretary as an option for defining EHBs • If so, the standards for the provision of coverage, including EHBs, would be met, as long as all EHB categories are covered • If not, states must select one of the base-benchmark plan options identified as defining EHBs.
Steps for Designing a Medicaid ABP (continued) • Step 3: Select a base benchmark plan to define the EHBs • Any of the three largest small group market health plans by enrollment • Any of the three largest state employee health benefit plans by enrollment • Any of the three largest federal employee health benefit plans by aggregate enrollment • The largest insured commercial non-Medicaid health maintenance organization operating in the state
Substitution Policy • Aligns with the individual and small group market • Allows flexibility for states to align benefit packages with their Medicaid state plan • Requires actuarial equivalence and placement in the same essential health benefit category
; Medicaid and Essential Health Benefits • Primarily Medicaid will align with EHB provisions in the individual and small group market. • States may use more than one EHB base benchmark to determine EHB coverage for Medicaid purposes • There are a few exceptions to address the specific needs of the Medicaid population
Prescription Drugs • The amount, duration, and scope of prescription drugs for an ABP is governed by the requirements of section 1937. • EHB prescription coverage standard: Provide at least the greater of: • 1 drug in every USP category and class; or, • Same # drugs in each category and class as EHB benchmark plan. • States must include sufficient prescription drug coverage to reflect the EHB benchmark plan standards at 45 CFR 156.122, including procedures in place that allow an enrollee to request and gain access to clinically appropriate drugs not covered by the plan. • To the extent that a prescription drug is within the scope of the ABP benefit as a covered outpatient drug, section 1927 and Federal rebates apply.
Habilitative Services and Devices • Coverage based on the habilitative services and devices that are in the applicable base benchmark plan • If habilitative services and devices are not in the applicable base benchmark plan, the state will define habilitative services and devices either in parity with rehabilitative services and devices or as determined by the state and reported to CMS in the ABP template
Preventive Services • EHB requirements for coverage of preventive services, including the prohibition on cost sharing, will apply to section 1937 ABPs
Medical Frailty • Definition of “medically frail” is modified and includes the addition of people with chronic substance use disorders • Individuals in the new adult group, if determined to be medically frail, will receive the choice of ABP defined using EHBs or ABP defined as state’s approved Medicaid state plan
Additional Items • States may include other benefits outside of 1905(a) described in sections 1915(i), 1915(j), 1915(k) and 1945 of the Social Security Act • All children under 21 enrolled in an ABP must receive Early and Periodic Screening, Diagnostic and Treatment (EPSDT), including pediatric oral and vision services • ABPs must also comply with the requirements of the Mental Health Parity and Addiction Equity Act (MHPAEA) • ABPs must include family planning services and supplies, FQHC/RHC services, and an assurance of NEMT
Transition • CMS is permitting transition time, if needed, as long as states are working toward, but have not completed a transition to the new ABPs on January 1, 2014.
1905(a) Preventive Services • CMS has codified changes to the definition of preventive services to be provided to the general Medicaid population • These changes do not relate to the provision of preventive services as an EHB • They relate to aligning the general 1905(a) definition of preventive services with the statutory construct at 1905(a)(13) of the Social Security Act • Services can be recommended by a physician or OLP
The Ryan White HIV/AIDS Program & Essential Health Benefits Health Resources & Services Administration, HIV/AIDS Bureau & Office of Planning, Analysis, and Evaluation Yolonda Campbell, Health Policy Analyst
Ryan White HIV/AIDS Program - still the Payer of Last Resort • “funds received…will not be utilized to make payments for any item or service to the extent that payment has been made, or can reasonably be expected to be made…” • Grantees and their subgrantees are expected to vigorously pursue enrollment in other funding sources (e.g., Medicaid, CHIP, Medicare, state-funded HIV/AIDS programs, employer-sponsored health insurance coverage, and other private health insurance) to extend finite RWHAP grant resources to new clients and/or needed services. • Once a client is enrolled in Medicaid or a private health plan, RWHAP funds may only be used to pay for items or services not covered, or partially covered, by Medicaid or the client’s private health plan (See PCN 13-01 & 13-04 at HAB’s Affordable Care Act website at http://hab.hrsa.gov/affordablecareact/). • RWHAP funds may also be used to cover the cost of premiums, deductibles, and co-payments for Medicaid and private health insurance (See PCN 13-05 and 13-06 at HAB’s Affordable Care Act website at http://hab.hrsa.gov/affordablecareact/).
RWHAP Core Medical and Support Services & Essential Health Benefits • Some RWHAP core medical (e.g, prescription drugs, mental health and substance abuse services) and support services (e.g, rehabilitation services) will be covered benefits under private health plans and Medicaid Alternative Benefit Plans. However, scope of coverage will vary by plan. • Some RWHAP core medical (e.g. adult oral health care) and many support services (e.g., treatment adherence counseling, outreach, transportation) may not be covered benefits under private health plans or Medicaid Alternative Benefit Plans • Grantees should understand the different benefit packages across private health plans and Medicaid alternative benefit plans so they can help clients identify and enroll in health coverage that best meets their individual HIV care needs. • Don’t forget that RWHAP funds may be used to pay for items or services not covered, or partially covered, by Medicaid or the client’s private health insurance plan.
Grantee Essential Health Benefits Package Resources • To learn about your state’s EHB-benchmark plan selection, please visit CCIIO’s EHB resource site at http://www.cms.gov/CCIIO/Resources/Data-Resources/ehb.html • CMCS will be posting information about your state’s EHB-benchmark plan for Medicaid Alternative Benefit Plans at the Medicaid.gov site (http://medicaid.gov/)
Health Coverage Options for PLWH AFTER the Affordable Care Act Employer-Based Insurance Health Insurance Marketplace Other Private Other Public Ryan White Program PLWH eligible for health coverage Cover comprehensive HIV medical and support services not covered, or partially covered, by public programs or private insurance Cover comprehensive HIV medical and support services not covered, or partially covered, by public programs or private insurance PLWH who remain uninsured
Helpful Affordable Care Act Resources • HealthCare.gov: https://www.healthcare.gov/ • HRSA, HIV/AIDS Bureau Affordable Care Act Website: http://hab.hrsa.gov/affordablecareact/ • Target Center: https://careacttarget.org/
Questions? If you have additional questions that were not answered in today’s webcast, please email RWP-ACAQuestions@hrsa.gov