Download

1 / 18
180 likes | 314 Views
Funding sources for health care: EU Structural Funds. Europe's health economies exchange. Financing regional healthcare workshop, AER, Katowice 19 March 2009. Professor Jonathan Watson PhD FRSM HCN Executive Director/Board of Trustees

E N D
Funding sources for health care: EU Structural Funds Europe's health economies exchange Financing regional healthcare workshop, AER, Katowice 19 March 2009 • Professor Jonathan Watson PhD FRSM • HCN Executive Director/Board of Trustees • Special Professor of Health & Public Policy, University of Nottingham Medical School • Governor – Edinburgh Napier University • External Partner- Bilbao Consortium (Deusto, Vilnius, Corvinus, Verona) • European Masters Degree in Sustainable Regional Health Systems
items • What NSRFs and OPs say • What regions want • Cost efficiency vs. cost effectiveness • EUREGIO III – its purpose and objectives
maximising health gains from Structural Funds Review of EU27 national strategic reference frameworks and operational programmes for DG SANCO and DG REGIO
Table 1 - Country assessment summary Table 2 - Eligible regions & Background Table 3 - Programme period 2007-2013, health investments in NSRFs and (R)OPs: financial allocations; NSRF strategic objectives; operational programmes; direct & indirect HS investments; evidence of capacity to deliver intersectoral policy & planning; regional planning & implementation; EC contacts Table 4 - Non health sector investments with potential health gains fiche format
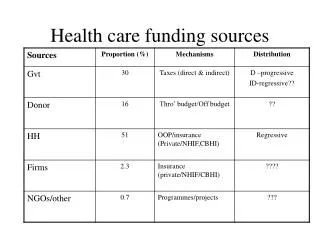
indirect health sector investment (€x bn - x.x%?) Others: Social inclusion, long-term care, public sector management, rehabilitation network, monitoring & research, medical tourism
non-health sector investment with potential health gain Integrated planning, one-stop shops (rural), health tourism, green spaces, procurement
Direct - There is little evidence about how (and if) the intended spend on health infrastructure will be achieved during the 2007-2013 period. In particular, what is not clear is if enough time has been invested in option appraisal to clearly inform investment planning and decisions. Indirect - A basic demographic challenge identified in most NSRFs is recognition that populations are ageing. This has led many EU MS to stress the need for creating diverse and flexible workforces across all sectors of society. Within the health sector and along the health sector supply chain there is a need to ensure that employment opportunities for vulnerable social groups are part of mainstream organisational human resources policy. Non-health sector - To maximise health gain from the knowledge economy there is a clear need to ensure that regional health systems, their organisations and staff are engaged in and contribute to knowledge hubs and innovation clusters. Good practice examples already exist that provide lessons on how this can be achieved e.g. TrusTech and Bionow (North West England), TSB Medici (Berlin), EUROSCAN, Medcon Ruhr and Human Technology Styria. key messages: investment areas
key messages: capacity to implement at regional level • Engagement of regional authorities in NSRF/OP/ROP planning and implementation as ROP Managing Authorities and/or Monitoring Committees (not in all MS) • But no clear attention to holistic capacity building in most of the newer EU12 e.g some mention of workforce development (e.g. Slovakia); holistic capacity building (Latvia); • New developments are mainly partnership focused: Regional Growth Forums (Denmark); Regional Sub-committees (Hungary); economic & social partners engaged in implementation (Netherlands); Regional coordination committee (Romania); bottom-up planning (Slovenia); regional development programmes (Sweden)
the need for practical “how to” knowledge and tools EUREGIO III - Health investments in Structural Funds 2000-2006: learning lessons to inform regions in the 2007-2013 period
EIII purpose and objectives • Review EUREGIO and agree best actions inclusion & assessment criteria - To review lessons learned from conduct of EUREGIO and other good practice sharing initiatives in order to build consensus about criteria for identifying and assessing good practices in use of Structural Funds for health investments. • Learning lessons from health investments - To identify examples of good practice and learn from problems experienced in planning, seeking funding for, implementing, evaluating and managing health investments in the 2000-2006 period: and 2007-2013 period when available. • Clarifying regional support needs – To undertake (i) a scoping and screening exercise of existing information, expertise and synergies (ii) a stakeholder analysis (iii) capacity building audits and case studies in paradigm regions in order to clarify existing and emerging regional support needs that will enable maximisation of health gains in three areas of SF investment (direct health sector, indirect health sector and non-health sector). • Opportunities and barriers to knowledge exchange - To undertake a gap analysis with key stakeholders in order to clarify how knowledge exchange about good practice can effectively be facilitated with & between (Regional) Operational Programme Managing Authorities, Monitoring Committees & SF beneficiaries. • Central access point and maximising uptake - To provide a centralised access point to practical 'what works' and 'how to' knowledge & coordinate activities to increase uptake and use of good practices and lessons learned in health investment by SF beneficiaries in EU regions.
EIII purpose and objectives 6. Dissemination - To stimulate exchanges and networking between EU27 regions that focus on the 'take home value' of good practice cases/themes/lessons and include communication methods that range from passive (publications, reports) to active (study visits, mentoring, workshops). 7. Sustainable outcomes for the 2007-2013 period and beyond - Build strategic linkages with key stakeholders & end users. EIII will support decision making across the spectrum of mainstream SF programmes in the current period; inform its mid-term review in terms of health gains maximized from SF investments; inform planning for the 2014-2020 period between relevant EC Directorates, national & regional Managing Authorities/Monitoring Committees and other key stakeholders and beneficiaries.
Associate Partners (HCN, European Centre for Health Assets & Architecture, Veneto Region, University of Maastricht, Liverpool University, EMK-Semmelweis University) Reference Group(National SF Managing Authorities for Hungary, Poland, Slovakia, Estonia, Bulgaria, Greece, Ruppiner-Kliniken/UMC representing Brandenburg, 4 other organisations representing former Objective 1 Regions) Collaborating partners (Assembly of European Regions, Regional Development Committee-European Parliament, EUROHEALTHNET, QeC-ERAN, EIB, EHMA, EUREGHA, European Association of Development Agencies) Stakeholders(EAHC, DG SANCO - C2 and C5, DG REGIO - D2 Thematic Development & Innovation, DG EMPLOY, DG ENTERPRISE) EIII connections
EIII work packages are interlinked and structured as follows: Assessment criteria - WP4 (scientific background), WP5 (inventory of case materials), WP6 (inventory of stakeholders, expertise and resources), WP7 (Website and knowledge database), WP8 (training materials package). Policy development - WP9 (master classes) WP2 (dissemination) bring together stakeholders informing them on the intermediate results of EIII. Assurance - WP10 (Reference Group) & WP2 (dissemination) deal with Assurance aspects as they enable discussion of emerging best actions evidence, its implications for health investments in the 2007-2013 period and for planning the 2014-2020 period. Evaluation - WP3 deals with internal and external evaluation aspects. EIII overview
health inequalities consultation: some thoughts • Can SF investments help reduce health inequalities? • Yes but improve the metrics used to assign SF • Where could spending be focused? • Job creation for local people • Capital for local food cooperatives • Housing improvement & renovation • Social capital (community centers, arts provision, adult education) • Better local schools
health inequalities consultation: some thoughts • What might be its impact? • Improved levels of human capital • Development of social capital • Healthier lifestyles • Improved levels of education • What can be done to share experience between regions? • Better use and connection with pan European local & regional networks • EU health programme, Structural Funds and Interreg • Emerging expertise • Ownership of exchange by regions and municipalities
final thoughts • Sustainable investment in EU12 MS regions needs to focus on capacity building as well as spending and outcomes • “One size fits all” does not work. Regions have different starting points. Evidence, policy and action might be better framed in two ways (i) common foundations (ii) regional clusters (cohesion objectives and/or ESPON categories) • Access to practical ‘know-how’ is a challenge but the critical challenge is how to use it in a chaotic environment.