Download
1 / 44
440 likes | 457 Views
Discover key components, strategies, and steps to enhance falls risk prevention programs for seniors. Learn clinical documentation enhancements and establish effective monitoring methods. Elevate coordination of care and prevent hospice patient falls effectively.

E N D
ing For You!Strategies to Strengthen a Falls Risk and Prevention Program Vivian Dodge, RN, BSN, MBA November 2012 Hospice of Palm Beach County
Objectives • Identify Components of a Falls Risk Prevention Program • Integrate a Falls Program in QAPI activities • Describe Various Strategies to Integrate the Falls Program in IDGs and Engage Staff • Identify Ways to Improve Clinical Documentation About Patient Falls
Falls Among Seniors… Why are they Important? • *1 in 3 adults 65 years of age and older fall each year*1 • For Seniors, falls are the leading cause of: • Injury • Hospitalization due to injury • Death due to injury • Previous falls are good predictors for future falls*2 • Nearly 95% of hip fractures result from falls *1 • Hospice patients: Increased risk for falls as patients decline and become more debilitated & frail • Coordination of care • *1 - AHRQ 2010 • *2 – Guide to Falls in Elderly, Dannemiller Memorial Education Foundation, 2003
The Base & BranchesSteps to “Grow” Your Program Adopt a Falls Risk Screening Tool Define goals Develop Definitions Collect Data Review Gaps Educate and Engage Establish PIP or Committee Ongoing Data Evaluation Provide Feedback Review Standards & Regulations
Steps to get on the right track • Establish the components for your Falls Program • Structure a PIP or committee • Identify challenges / opportunities • PDCA ! • Evaluate data & outcomes and continually re-evaluate the effectiveness of your program
Branch 1: Requirements • Review standards & regulations • Jt Commission, CHAPS, ACHC • State regulations / standards • Review standards of practice • Related associations • NHPCO, HPNA, NAHC, etc • Review research • AHRQ, CMS, OASIS, IOM, Nat’l Center for Patient Safety
Branch 2:The Workgroup or PIP is Essential Determine membership: Variety, good cross section, creative, committed Define the purpose & goals: What do you want to accomplish Determine frequency of meetings, data for review, other actions: How soon can data be provided? Too frequently or too little affects momentum Determine reporting chain of command: Who? Who are the persons/departments that have in interest in the outcomes? Various levels?
Branch 3:Specifications • Define goals – what is it that you want to accomplish? • What is your organization fall rate? • Define the elements: > What is the organization definition of falls? • What kind of data will you collect?
Branch 4:The Screening Tool • Adopt a screening tool to assess for patients’ risk for falls Morse Falls Scale Hendrick Falls Scale Falls Efficacy Scale Many others !! Provides standardization in scoring
Screening Tools • Provides standardization among clinical staff • Assists with development of practice standards and interventions in your organization • Reliability • Becomes part of assessment documentation
Branch 5:Protocols & Interventions • Specify when screening is completed & frequency • What actions clinical staff take if patient is identified at risk for falls • Determine documentation expectations of falls risk • Determine documentation expectations of any falls • Review incident reporting forms • Communication & visual identification
Branch 6:Education • Education of patients/families/caregivers is critical • Engage them in learning • Education of staff is imperative Engagement promotes : -Greater understanding -Better compliance -Improved collaboration & coordination of care -Improved outcomes information REINFORCEMENT
Challenges & Opportunities • Workgroup started in 2006 • Lack of understanding by clinical staff what the Falls Program really meant • Lack of documentation about the fall event • Poor reporting compliance and lack of information on incident reports • Staff did not report falls from SNFs
Challenges & Opportunities • Staff not well versed on interventions available nor appropriate education • Fear of Reporting • Lack of understanding of why it is important to report • Ideas that QM department is responsible • Lack of understanding of importance related to future clinical outcomes and regulatory compliance • WIIFM?
Data Determine detail of data • Number of falls • Attended / Unattended • Injury status: No injury, Minor injury, Fractures, Death • 911 calls • Time of event • Category of fall • Frequent Fallers • Team & Region • Treatment
Data • Diagnosis • Fall Risk Score • Disposition of patient • Year to date data • Quarterly Fall Rate • Fiscal Year Comparisons
Here’s What We Found • Most falls occur during the day • Top 4 categories: Found on Floor Rolled out of Bed Bathroom / toileting related Ambulation • Majority of falls - No injury • Majority of falls in home environment or ALFs • Inpatient units – low fall rates • Lack of documented follow up for falls with injuries to the head
Here’s What We Found: 5Falls Risk • Hospice patients with polypharmacy – interactions, efficacy • Types of medications: Diuretics & laxatives – sense of urgency Anti-hypertensive meds, sedatives, narcotics- Sleeping, pain & blood pressure medications can cause hypotension and effect alertness Psychoactive drugs (Haldol, Seroquel) - increase risk for falls • Chronic pain and musculoskeletal pain in 2 or more joints & pain interfering with ADLs – more likely to fall • Delirium- more likely to fall
Here’s What We Found: • Staff not well versed on DME available – products, knowledge • Lack of collaboration with facilities to implement interventions for fear of ‘stepping on their toes’ –What is allowed? Education needed of how hospices can assist? • Language used by clinical staff – How staff present information • Lack of toileting routines – sense of urgency, increased falls
Here’s What We Found: • Poor eyesight, hearing – increased falls • Patients/families did not want equipment – unsightly and gave impression of fragility • Missing hand off communication – contributes to lack of clinical follow up
PDCA – Plan, Do, Check, ActAway We Go! • Reviewed ongoing gap analysis • Provided monthly feedback to teams on falls • Discussed at Quarterly Quality Meetings • Developed audit tools • Developed yearly initiatives for Falls Workgroup • Attended IDGs • Reviewed medical records and provided feedback to supervisors and nurses • Evaluated data • Developed patient teaching handouts • Developed staff teaching handouts • Provided education to staff
Keeping the Momentum Keeping “Falls” activities on staff radar has been challenging but became a successful endeavor Data is boring Workgroup was committed to having fun
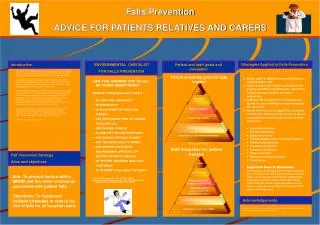
Patient safety begins with HPBC’s Fall Prevention Program Falling For You! PREVENT YOUR PATIENT FROM BECOMING A FALLING STAR • FALLS AMONG SENIORS • 1 of every 3 people over the age of 65 fall a year • For Seniors, falls are the leading cause of: • -Injury • -Hospitalizations • -Death due to injury • Remember To: • Use the Fall Stickers • Use the Fall Stickers on the patient folders in the home • Update Care Plans • Educate Patient / Family / Caregiver
Into Action! • HPBC Facts • Average 115-130 falls per month • Fall Rate Less than 1% of HPBC Patients • (That’s Good!) • February Facts: • 54% of February 08 falls occurred during the day • 14% occurred in the evening • 25% occurred during the night • Most Falls Occurred Unattended in the Homes • Only 6 Serious Injuries (Fractures –Mostly Hip FX’s) Patient safety begins with HPBC’s Fall Prevention Program Remember To: Use the Fall Stickers Use the Fall Stickers on Patient Folders in the Home Update the Care Plans Educate the Patient / Family / Caregiver
Patient safety begins with HPBC’s Fall Prevention Program Summer Star Gazing Looking for Falling Stars GOAL: Keep HPBC fall rate to < 1% of patient days :Currently at 0.41% • Educate, Educate, Educate! Proper Body Mechanics • How to use DME Equipment Safely • Fall Prevention Tips • Paint the Picture • Who? • What? • Where? • When? • Why? • How? Good Job To All On: Updating the Care Plans Good IR reporting
FALLS: TO M.E. OR NOT TO M.E. How do you know when to contact the Medical Examiner’s Office if there was a fall? Simple Rule of Thumb • Did the fall/trauma contribute or hasten an unnatural death? • Did the patient’s status, or mentation change as a result of the fall? • Example: Patient was ambulating, talking prior to fall; now patient is unresponsive • Example: patient active prior to fracture of hip. Since fracture, patient is bedridden • Was the patient’s lifestyle changed due to the event? • Did the fall result in fractures from which patient did NOT recover? • (Fx hips, femurs, etc) • Did the patient die of complications from the fracture or fall? • Example: Pt developed pneumonia or embolism post fall • Important: Was patient already declining or pre-imminent prior to the fall? If yes, then may not be a ME case.
Laws Governing Medical Examiner Cases: • FLA Statute 406.11; Gives authority to Medical Examiner • to do an autopsy in suspicious deaths • FLA Statue 406.12: Duty to Report – specifies health care workers • have a duty to report suspicious deaths • There are many reasons patients are M.E. cases…. • But today, we are only focusing on Falls and M.E. cases • What to do? • What to do? • Discuss with team physician events surrounding the fall • If uncertain: Always good to discuss case with ME office. • Use the Medical Examiner Worksheet as a guide and place in chart • Document all calls and conversations with the ME office. • Remember: ME office has final jurisdiction • Discuss patient’s condition pre and post fall
Guess what’s coming your way?TT / FFHint: It’s not True and FalseFrom your HPBC Falls Workgroup TT FF
Barriers to Changing Patient Behavior Fear Changing what is familiar Wanting to stay independent Not aware of DME options and how it can benefit Afraid of appearing old or frail Afraid of what appears new or confrontational Not ready to accept decline/mortality Do not like how DME takes up space in the home
Positive Reinforcement Goes a Long Way • Stay patient with your patients • Engage a family member, caregiver • Teach how to operate equipment or transfer patient: Use the teaching techniques! • Staff too!
Other Actions • Clinical staff education > DME possibilities: Hi/lo beds, mats, transfer boards, etc > Feedback on audits > Feedback on Plan of Care expectations > Feedback on documentation
So… How Did We Do? Outcomes: Continued Reduction in Falls Rate 38% reduction
Benchmarking • Little comparative data on falls in the hospice industry • Home health, acute hospitals collecting data for years • Future? Required reporting? • NHPCO initiatives
Our Falling Stars Establish process/protocols Educate Engage Question Quantify Quality check
References: -National Quality Measures Clearinghouse, www. qualitymeasures.ahrg.gov -Agency for Health Research and Quality (AHRQ), www.ahrg/qual Institute of Medicine National Academies, IOM, www.iom.edu -The Joint Commission of Healthcare Organizations, CAMH, 2012 -National Center for Patient safety, Department of Veterans Affairs, www.patientsafety.gov -National Institute on Aging, www.nia.nih.gov -”Engaging patients and Families in the Quality and Safety of Hospital Care”, AHRQ, June 2012 -Guide to the prevention and management of Falls in the Elderly, Dannemiller Memorial educational foundation & McMahon Publishing Group, 2003 -“Etiology of Falls among Cognitively Intact Hospice Patients”, Schonwetter, Kim, Kirby, Martin, Henderson, Journal of Palliative Medicine Vol. 13, No. 11, 2010 -
Thank you! Questions? Vivian Dodge, RN, BSN, MBA Hospice of Palm Beach County Office: 561-227-5171 Email: vdodge@hpbc.com