Download
1 / 57
800 likes | 1.94k Views
The Ottawa Model of Research Use. Ian D Graham, PhD Canadian Institutes of Health Research School of Nursing, UOttawa Sept. 24, 2007. What do we know about research use?. Uptake of research influenced by: Perceptions of the innovation- (ie the evidence, CPGs) The potential adopter

E N D
The Ottawa Model of Research Use Ian D Graham, PhD Canadian Institutes of Health Research School of Nursing, UOttawa Sept. 24, 2007 University of Ottawa/ CIHR
What do we know about research use? • Uptake of research influenced by: • Perceptions of the innovation- (ie the evidence, CPGs) • The potential adopter • The practice setting or social context University of Ottawa/ CIHR
Factors influencing uptake of innovations: The Innovation • Development process • Attributes of the innovation University of Ottawa/ CIHR
Development Process • Credible developers • all relevant stakeholders • interdisciplinary • Objective & rigorous method • Careful documentation • explicit & transparent process • Local involvement University of Ottawa/ CIHR
Characteristics of the Innovation • Relative advantage (useful) • Low complexity (ease of use or do) • Compatible • (fits with current practice, norms/values) • (does not demand change in existing practice) • Trialability (easy to try) • Clear (not vague or non-specific) • Evidence-based • Re-invention • (Rogers 1995) (Grilli and Lomas, 1994) (Grol et al 1998) (Foy et al 2003) University of Ottawa/ CIHR
Factors influencing uptake of innovations: Potential Adopters • awareness • attitudes • knowledge/skill • concerns • current practice/habit University of Ottawa/ CIHR
Factors influencing uptake of innovations: Practice Environment- Structure Factors • Decision-making • Policies, rules, laws • Available technology: equipment, testing • Physical layout • Work pressure (info overload, competing demands, no time, chaotic environment) • Human resources University of Ottawa/ CIHR
Practice Environment: Culture/social Factors • Culture & belief systems • Norms, institutionalized habits • Leadership • Politics & personalities • Peer influence University of Ottawa/ CIHR
Practice Environment: Other Factors • Patients/Consumers • Case mix, behavior, attitudes, preferences & demands • Economic Considerations • Resources, remuneration, funding systems • Medical/Legal Issues • Other Organizational/System Factors University of Ottawa/ CIHR
What do we know about the effectiveness of implementation interventions? • Cochrane’s EPOC (Effective Practice and Organization of Care) Group • Systematic reviews of: • Professional interventions (e.g. continuing medical education, audit and feedback) • Organizational interventions (e.g. the expanded role of pharmacists) • Financial interventions (e.g. professional incentives) • Regulatory interventions University of Ottawa/ CIHR
Little or no effect Educational materials* Didactic educational meetings Sometimes effective Audit and feedback Local opinion leaders Local consensus processes Patient mediated interventions Effectiveness of Knowledge Translation/implementation Interventions (Bero et al., 1998, Grimshaw et al., 2001, Grimshaw, 2004) University of Ottawa/ CIHR
Generally Effective • Educational outreach visits • Reminders • Interactive educational meetings • Multifaceted interventions including two or more of: • Audit and feedback • Reminders • Local consensus processes • Social marketing University of Ottawa/ CIHR
Summary of Reviews on KT/Implementation Interventions • No magic bullets- most interventions effective under some circumstances, none effective under all circumstances • Multiple ongoing interventions are usually necessary • Evidence is sparse for many interventions University of Ottawa/ CIHR
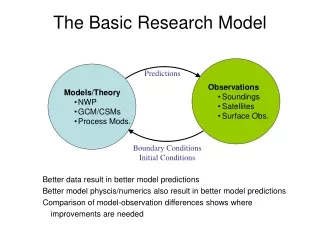
How Can We Facilitate Knowledge to Practice? • Need a Conceptual Framework to Guide Implementation • Planned action vs classic theories of change University of Ottawa/ CIHR
Ottawa Model of Research Use Assess + Monitor + Evaluate Innovation Potential Adopters Interventions • Adoption • Outcomes • Practice Environment University of Ottawa/ CIHR
Getting Started • Who is wanting to bring about the change in practice? Where are they located in the social system? • What is their jurisdiction & scope of activities they can perform? • What are their strategic alliances? • What resources are available? • Who is going to be the change agent(s)/facilitator(s)? University of Ottawa/ CIHR
Ottawa Model of Research Use Assess + Monitor + Evaluate barriers & supports interventions outcomes & degree of use Innovation (CPG, tools) Potential Adopters Interventions Adoption Outcomes Practice Environment University of Ottawa/ CIHR
Ottawa Model of Research Use Assess + Monitor + Evaluate barriers & supports interventions outcomes & degree of use • Innovation • Implementation • Interventions • barrier • management • transfer • follow-up Potential Adopters Outcomes Adoption Practice Environment University of Ottawa/ CIHR
Ottawa Model of Research Use Assess + Monitor + Evaluate barriers & supports interventions outcomes & degree of use • Innovation (guideline) • development process • innovation attributes • Potential Adopters • awareness • attitudes • knowledge/skill • concerns • current practice • Interventions • barrier • management • transfer • follow-up • Adoption • intention • use • sustained use • Outcomes • patient • practitioner • system • Practice Environment • structural • culture/social • patients • economic University of Ottawa/ CIHR
Ottawa Model of Research Use Assess + Monitor + Evaluate barriers & supports interventionsoutcomes & degree of use • Innovation • development process • innovation attributes • Potential Adopters • awareness • attitudes • knowledge/skill • concerns • current practice • Outcomes • patient • practitioner • system • Interventions • barrier • management • transfer • follow-up • Adoption • intention • use • sustained use • Practice Environment • structural • culture/social • patients • economic University of Ottawa/ CIHR
Additional References • Logan J, Graham, ID. Toward a Comprehensive Interdisciplinary Model of Health Care Research Use. Science Communication 1998;20(2):227-246. • Graham ID, Logan J. Innovations in knowledge transfer and continuity of care. Can J Nurs Res. 2004 Jun;36(2):89-103. • RNAO Implementation of Practice Guidelines Toolkit http://www.rnao.org/bestpractices/PDF/BPG_Toolkit.pdf • Grimshaw et al 2004. Systematic review of the effectiveness and efficiency of guideline dissemination and implementation strategies. Htpp://www.ncchta.org/project.asp?PjtId=994 University of Ottawa/ CIHR
Adoption and sustainability of decision support for patients facing health decisions: An implementation case study with embedded RCT Dawn Stacey RN PhD Assistant Professor, University of Ottawa Funding: Canadian Institutes of Health Research September 2007 University of Ottawa/ CIHR
Outline • Background • Purpose & Objectives • Theoretical Framework • Methods • Results • Implications for Research, Education and Practice University of Ottawa/ CIHR
Public’s view on who should make risk-related health decisions (Magee, WHO, 2003) University of Ottawa/ CIHR
Problem: Decisional Conflict • uncertainty about which course of action to take North American Nursing Diagnosis Association, 2002 yes no University of Ottawa/ CIHR
‘Innate’ contributing factors 2 or more options Outcomes: risky/uncertain, permanent, serious Value tradeoffs: benefits versus harms Anticipated regret: ‘missed’ benefits of option not chosen regret University of Ottawa/ CIHR
Consequences: unresolved decisional conflict & related factors • 59 timesmore likely tochange mind • 23 timesmore likely todelay decision • 5 timesmore likely tohave regret • 3 timesmore likely tofail knowledge test • 19%more likely toblame practitioner for bad outcomes (Sun, Q. [MSc thesis]. University of Ottawa, 2005; Gattelari & Ward J Med Screen 2004;11:165-169) University of Ottawa/ CIHR
Improve decision quality 15% higher knowledge scores 70% more realistic expectations (probabilities) better match between values & choices Reduce decisional conflict (9 points) Help undecided to decide (50%) Patients 40% less passive in decisions Reduce over-use -25% surgery; -20% PSA; -29% HRT Potential to reduce under-use Compared to standard care, patient decision aids… O’Connor et al., Medical Decision Making, 2007 University of Ottawa/ CIHR
Value of coaching [hysterectomy] (Kennedy et al. JAMA 2002; 288: 2701-2708) University of Ottawa/ CIHR
Framework for Decision Coach-Mediated Shared Decision Making Primary Clinician Role to diagnose patient problem; discuss options; screen for decisional conflict; refer for decision support Patient Role Communicate informed values & priorities shaped by their social circumstances Goal: Informed decision making based on patients’ priorities & values • Decision Coach Role • (Ottawa Decision Support Framework) • Assessing decisional needs • Providing decision support tailored to needs • Monitoring & facilitating progress in resolving needs and decision quality • Screen for implementation needs University of Ottawa/ CIHR (Stacey, Murray et al., Worldviews on Evidence-based Nursing in press)
Client Centred Care “Providing care that is respectful of and responsive to individual patient preferences, needs and values and ensuring that patient values guide all clinical decisions”(p.6, Institute of Medicine, 2001) RNAO Nurse Best Practice Guideline: Client Centred Care (2006) “Nurses have a central role in providing clinical expertise to facilitate clients’ decision making…to reach decisions that are well-informed and best for them” (p.3) • Involve clients in decision making • Provide structured decision support using patient decision aids and decision coaching University of Ottawa/ CIHR
Purpose of research A case study with an embedded randomized controlled trial (RCT), guided by the Ottawa Model of Research Use • To explore baseline barriers and facilitators re decision support/coaching by call centre nurses • To design and evaluate a multifaceted intervention to improve the quality of nurses’ decision support • To describe the uptake and sustainability of decision support by call centre nurses Ethics approval by University of Ottawa, Research Ethics Board University of Ottawa/ CIHR
BCNurseLine call centreServes population of 4.2 million since 2001 • Goal • To help BC residents manage personal health issues and make ‘sound’ health decisions • Healthwise® Knowledgebase resources • Public access to a handbook and internet-based health information including 95+ patient decision aids • Concurrent initiatives Dec 03 to June 04 • Major reorganization of nurse supervisors positions • Imminent contract renewal for call centre services • High absenteeism increased call pressure University of Ottawa/ CIHR
Decision Point Top Hits at BCNurseLine • Breast or bottle feeding • Birth control method • Treatment for miscarriage • Removing wisdom teeth • Amniocentesis • Antibiotics for acute bronchitis (884 hits total for 2003) University of Ottawa/ CIHR
Ottawa Model of Research Use 1. Baseline assessment 2. RCT of intervention 3. Uptake & sustainability Assess + Monitor + Evaluate barriers & facilitators interventions outcomes & degree of use Innovation Decision support • Multifaceted intervention • online autotutorial • decision support /coaching protocol • skill workshop • performance feedback • Potential Adopters: • Nurses • awareness • attitudes • knowledge/skill • confidence • current practice • Outcomes • patient • practitioner • system • Adoption • intention • use • Practice Environment • BCNurseLine • organization’s policies, mandate • callers (Logan J & Graham ID, 1998; Graham ID & Logan J 2004) University of Ottawa/ CIHR
Case study method (Dec ‘03 to June ‘04) Analysis • Conceptual content analysis of qualitative data • Descriptive analysis of surveys; t-tests and ANCOVA for trial data • Triangulation of results across data sources University of Ottawa/ CIHR (Creswell JW, 1998; Sidani S & Braden CJ, 1998; Yin R, 2003)
RCT methods 41 call centre RNs December 2003 41 simulated calls* 21 Intervention (knowledge test; acceptability surveys) Stratified by FTE status R February 2004 20 Control (knowledge test) April 2004 19+ simulated calls 20 simulated calls (* Missed taping 1 call; + 2 dropped at the beginning of the intervention) 12 intervention May 2004 University of Ottawa/ CIHR
Characteristics of participants % University of Ottawa/ CIHR
Baseline facilitators for nurses providing decision support/coaching • Innovation: • Access to >95 patient decision aids • Potential adopters: Nurses • Positive attitudes • Already refer to patient decision aids • Recognize callers having difficulty with decisions • Practice Environment: Call centre infrastructure • supervisors/educators • classification of calls (Stacey, Graham, O’Connor, Pomey. Worldviews Evidence-based Nursing, 2005: 2: 184-195) University of Ottawa/ CIHR
Key Elements of Quality Decision Support Provided by Nurses to Simulated Callers (N=38) University of Ottawa/ CIHR
Baseline barriers to nurses providing decision support • Innovation: • Inefficiency to find/use decision aids in database • No structured process to guide calls • Potential adopters: Nurses • Lack knowledge, skill, confidence • Practice Environment: Call centre infrastructure • Unclear program mandate • Organizational pressure to minimize call length • Low public awareness of call centre services University of Ottawa/ CIHR
Multifaceted intervention to address baseline barriers (Grimshaw J, et al., 2001 & 2004; Thomas L, et al., 1999) University of Ottawa/ CIHR
Decision support protocol A process for coaching clients making decisions with 2 or more options Available at www.ohri.ca/decisionaid Based on: Ottawa Decision Support Framework University of Ottawa/ CIHR
RCT to Enhance Nurse Decision Support Coaching Time in Minutes (Stacey et al., 2006, J Telemed & Telecare) University of Ottawa/ CIHR
Health professionals’ decision support knowledge % (Stacey et al., 2006, J Telemed & Telecare; Stacey et al., ISCCN, 2006)
Coaches’ decision support skills improve(simulated calls) Mean quality scores p < 0.001 (Stacey et al., 2006, J Telemed & Telecare; Stacey et al., ISCCN, 2006)
Adoption of decision support • 25 of 31 trained nurses completed the survey • Of 25 nurses, • 23 plan to use decision support protocol next 3 months • 21 felt comfortable using it • 11 already used it with callers • 14 did not receive an appropriate call • “It was just plunge in, see what you do the first time…And I may not have been right on all of them but I could see where I missed. The next one I thought was better.” (Stacey et al., Implementation Science, 2006) University of Ottawa/ CIHR
Use with real callers: comments • Recognized the need for decision support “It was a medication call and she had quite a few questions. But underlying it all, was her concern about how to select birth control.” • Felt better prepared “I’m more likely to ask questions about the decision … instead of just making assumptions, which is a lot of what I did earlier.” • Felt positive about their practice “I used to feel quite nervous that …I felt like I should know the answer. So this has given me a lot of power that you can help them, that you don’t have to sort it out for them.” University of Ottawa/ CIHR