Download
1 / 1
10 likes | 100 Views
Association between eosinophilic airway inflammation and T-cells response in children with bronchial asthma. J. Antipkin 1 , T. Umanets 1 , V. Lapshyn 1 , A. Nakonechna 2. Abstract 2160. Institute of Pediatry, Obstetrics and Gynaecology, Kiev, Ukraine

E N D
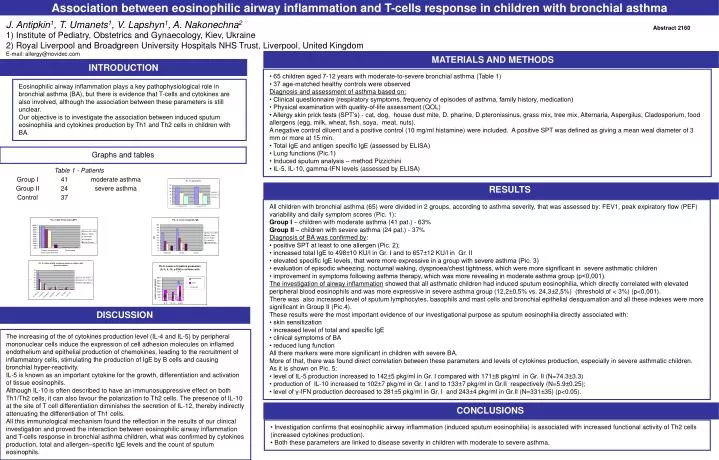
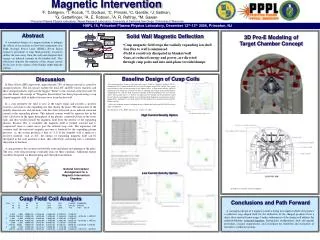
Association between eosinophilic airway inflammation and T-cells response in children with bronchial asthma J. Antipkin1, T. Umanets1, V. Lapshyn1, A. Nakonechna2 Abstract 2160 • Institute of Pediatry, Obstetrics and Gynaecology, Kiev, Ukraine • Royal Liverpool and Broadgreen University Hospitals NHS Trust, Liverpool, United Kingdom • E-mail: allergy@novidec.com MATERIALS AND METHODS INTRODUCTION • 65 children aged 7-12 years with moderate-to-severe bronchial asthma (Table 1) • 37 age-matched healthy controls were observed Diagnosis and assessment of asthma based on: • Clinical questionnaire (respiratory symptoms, frequency of episodes of asthma, family history, medication) • Physical examination with quality-of-life assessment (QOL) • Allergy skin prick tests (SPT’s) - cat, dog, house dust mite, D. pharine, D.pteronissinus, grass mix, tree mix, Alternaria, Aspergilus, Cladosporium, food allergens (egg, milk, wheat, fish, soya, meat, nuts). A negative control diluent and a positive control (10 mg/ml histamine) were included. A positive SPT was defined as giving a mean weal diameter of 3 mm or more at 15 min. • Total IgE and antigen specific IgE (assessed by ELISA) • Lung functions (Pic.1) • Induced sputum analysis – method Pizzichini • IL-5, IL-10, gamma-IFN levels (assessed by ELISA) Eosinophilic airway inflammation plays a key pathophysiological role in bronchial asthma (BA), but there is evidence that T-cells and cytokines are also involved, although the association between these parameters is still unclear. Our objective is to investigate the association between induced sputum eosinophilia and cytokines production by Th1 and Th2 cells in children with BA. Graphs and tables All children with bronchial asthma (65) were divided in 2 groups, according to asthma severity, that was assessed by: FEV1, peak expiratory flow (PEF) variability and daily symptom scores (Pic. 1): Group I – children with moderate asthma (41 pat.) - 63% Group II – children with severe asthma (24 pat.) - 37% Diagnosis of BA was confirmed by: • positive SPT at least to one allergen (Pic. 2); • increased total IgE to 498±10 KU/l in Gr. I and to 657±12 KU/l in Gr. II • elevated specific IgE levels, that were more expressive in a group with severe asthma (Pic. 3) • evaluation of episodic wheezing, nocturnal waking, dyspnoea/chest tightness, which were more significant in severe asthmatic children • improvement in symptoms following asthma therapy, which was more revealing in moderate asthma group (p<0,001). The investigation of airway inflammation showed that all asthmatic children had induced sputum eosinophilia, which directly correlated with elevated peripheral blood eosinophils and was more expressive in severe asthma group (12,2±0,5% vs. 24,3±2,5%) (threshold of < 3%) (p<0,001). There was also increased level of sputum lymphocytes, basophils and mast cells and bronchial epithelial desquamation and all these indexes were more significant in Group II (Pic.4). These results were the most important evidence of our investigational purpose as sputum eosinophilia directly associated with: • skin sensitization • increased level of total and specific IgE • clinical symptoms of BA • reduced lung function All there markers were more significant in children with severe BA. More of that, there was found direct correlation between these parameters and levels of cytokines production, especially in severe asthmatic children. As it is shown on Pic. 5: • level of IL-5 production increased to 142±5 pkg/ml in Gr. I compared with 171±8 pkg/ml in Gr. II (N=74.3±3.3) • production of IL-10 increased to 102±7 pkg/ml in Gr. I and to 133±7 pkg/ml in Gr.II respectively (N=5.9±0.25); • level of γ-IFN production decreased to 281±5 pkg/ml in Gr. I and 243±4 pkg/ml in Gr.II (N=331±35) (p<0.05). RESULTS The increasing of the of cytokines production level (IL-4 and IL-5) by peripheral mononuclear cells induce the expression of cell adhesion molecules on inflamed endothelium and epithelial production of chemokines, leading to the recruitment of inflammatory cells, stimulating the production of IgE by B cells and causing bronchial hyper-reactivity. IL-5 is known as an important cytokine for the growth, differentiation and activation of tissue eosinophils. Although IL-10 is often described to have an immunosuppressive effect on both Th1/Th2 cells, it can also favour the polarization to Th2 cells. The presence of IL-10 at the site of T cell differentiation diminishes the secretion of IL-12, thereby indirectly attenuating the differentiation of Th1 cells. All this immunological mechanism found the reflection in the results of our clinical investigation and proved the interaction between eosinophilic airway inflammation and T-cells response in bronchial asthma children, what was confirmed by cytokines production, total and allergen–specific IgE levels and the count of sputum eosinophils. • Investigation confirms that eosinophilic airway inflammation (induced sputum eosinophilia) is associated with increased functional activity of Th2 cells (increased cytokines production). • Both these parameters are linked to disease severity in children with moderate to severe asthma. CONCLUSIONS DISCUSSION

![>> W1=[1 1 1 1;1 -j -1 j;1 -1 1 -1;1 j -1 -j] W1 =](https://cdn1.slideserve.com/3227081/slide1-dt.jpg)