Download
1 / 37
400 likes | 493 Views
Explore the intricate mechanisms of insulin, glucagon, and somatostatin in the regulation of blood glucose and metabolic processes in the pancreas. Learn about the causes, signs, and symptoms of hyperglycemia as well as the complications of diabetes mellitus.

E N D
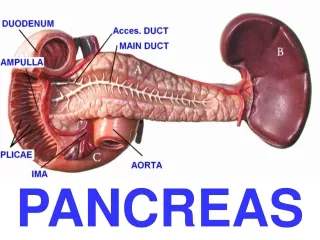
PANCREAS • INSULIN • GLUCAGON • SOMATOSTATIN
INSULIN – STRUCTURE • peptide • low species variability (ie. Porcine and human insulin – 1 AA is different) • half life 5-8 minutes • degradation in liver and kidneys
BLOOD GLUCOSE REGULATION INSULIN AND GLUCAGON
STIMULATION Increased glucose Increased AA Increased fatty acids Gastrin Cholecystokinin Glucagon Epinephrine Parasympathetic system INHIBITION Decreased glucose Decreased AA Decreased fatty acids somatostatin INSULIN –REGULATION OF SECRETION
INSULIN - LIVER • Increased glucose uptake • Stimulation of glycogenogenesis • Stimulation of glycolysis • Inhibition of gluconeogenesis • Increased fatty acids and very low density lipopoteins (VLDL) synthesis
INSULIN - MUSCLES • Increased glucose uptake • Stimulation of glycogenogenesis • Stimulation of glycolysis • Stimulation of aminoacids transport • Stimulation of protein synthesis
INSULIN - ADIPOCYTES • Increased glucose uptake • Stimulation of glycolysis • Stimulation of α-glycerol phosphate synthesis • Inhibition of lipolysis
STIMULATION Decreased glucose Decreased AA Exercise Stress Sympathetic system INHIBITION Insulin Increased glucose Somatostatin GLUCAGON –REGULATION OF SECRETION
GLUCAGON – METABOLIC EFFECTS • LIPIDS • Oxidation of fat in hepatocytes => ketones => alternate to glucose fuel • Release of FA from adipocytes • CARBOHYDRATES • Stimulation of glycogenolysis • Stimulation of gluconeogenesis • Increased FA => inhibition of glucose uptake by muscles and adipocytes • PROTEINS • AA uptake into liver => gluconeogenesis • Activation of liver urea cycle
SOMATOSTATIN • 14-aminoacid peptide • produced in delta cells of pancreas (also in GI tract, hypothalamus) Releasestimulated by: • glucose • aminoacids • fattyacids • secretin • cholecystokinin Actions: • decreasesgutmotility • inhibitsrelease of gastrin, secretin, cholecystokinin • decreasesgastricacidsecretion • decreasesgastricemptying • decreasesgallbladercontraction • suppresses insulin and glucagonrelease • suppressesgrowthhormonerelease
Pathogenesis of hyperglycemia. 1, Glycogenolysis. 2, Gluconeogenesis. 3, Reduced uptake of glucose-contributing hyperglycemia. 4, Glucosuria. 5, Lipolysis. 6, Proteolysis. 7, Fatty acid metabolism. Acetyl CoA, acetyl coenzyme A; glucose-6-P, glucose-6-phosphate; TCA, tricarboxylic acid; TG, triglycerides.
Causes of Hyperglycemia • Diabetesmellitus • Endocrinehyperfunctionsyndromes • Glucagonoma • Cushing’ssyndrome • Growthhormonehypersecretion • Thyrotoxicosis • Pheochromocytoma • Acutepancreatitis • Drugs • Thiazidediuretics • Phenytoin • Hormones (e.g., cortisone, thyroxin)
Signs and Symptoms of Hyperglycemia • Glucose increased in blood, urine, and body fluids • Polyuria—nocturia • Dehydration—dry mouth, skin, and mucosae • Polydipsia and increased thirst • Polyphagia and feeling of hunger • Weight loss/gain • Fatigue, nausea • Blurry vision and headaches • Pruritus vulvae or balanitis due to Candida albicans • Mood change, irritability, apathy
Causes of Hypoglycemia Major organ failure Liver failure Kidney failure Heart failure Systemic diseases Multiple organ failure Sepsis Malnutrition Alcoholism Childhood inborn errors of metabolism • Diabetes therapy related • Insulin • Sulfonylurea • Tumors secreting insulin or IGF • Insulinoma • Sarcomas • Carcinoma of liver, kidneys, adrenal glands • Drugs • Pentamidine • Sulfonamides • Salicylates
Classification of Diabetes Mellitus (DM) • Type 1 DM (absolute insulin deficiency due to beta cell destruction) • Type 2 DM (insulin resistance and relative insulin deficiency) • Other types of DM • Genetic defects involving islet cells, insulin receptors, etc. • Genetic and chromosomal syndromes (e.g., Down, Turner’s, and Klinefelter’s) • Pancreatic diseases and pancreatectomy • Systemic diseases (e.g., hemochromatosis, autoimmune endocrine insufficiency) • Excess of insulin antagonizing hormones (e.g., glucagons, corticosteroids, growth hormone, thyroid hormones) • Drug-induced DM (e.g., thiazide diuretics)
Comparison of Coma due to Diabetic Ketoacidosis and Hyperosmolar Nonketotic Diabetes Mellitus (DM)
DIABETES MELLITUS - COMPLICATIONS • ACUTE • Ketoacidosis • Polyuria • Dehydration • Hyperosmolar coma • CHRONIC • Microangiopathy • Macroangiopathy • Neuropathy • Nephropathy • Ulcerations • Hyperlipidemia • Protein wasting