Download
1 / 21
210 likes | 231 Views
Chapter 23: The Thyroid Gland. By Marissa Grotzke. The Thyroid. Produces 2 hormones Thyroid hormone: critical in regulating body metabolism, neurologic development, & other functions Calcitonin: secreted by parafollicular C cells & involved in calcium homeostasis

E N D
Chapter 23: The Thyroid Gland By Marissa Grotzke
The Thyroid • Produces 2 hormones • Thyroid hormone: critical in regulating body metabolism, neurologic development, & other functions • Calcitonin: secreted by parafollicular C cells & involved in calcium homeostasis • Conditions affecting thyroid hormone levels are much more common than those affecting calcitonin.
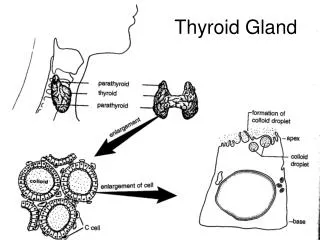
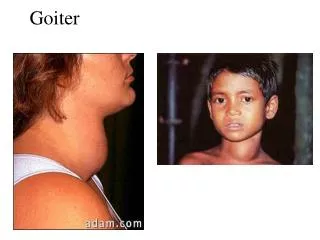
The Thyroid • Thyroid Anatomy and Development • Positioned in lower anterior neck & shaped like a butterfly • Made up of 2 lobes that rest on each side of trachea; band of thyroid tissue (isthmus) runs anterior to trachea & bridges lobes • Parathyroid glands: posterior to thyroid; regulate serum calcium levels & recurrent laryngeal nerves that innervate vocal cords • Thyroid hormone is critical to neurologic development of fetus. • Iodine is an essential component of thyroid hormone; iodine deficiency leads to hypothyroidism, mental retardation, cretinism (stunted physical and mental growth). • Congenital hypothyroidism occurs in 1 of 4,000 live births.
The Thyroid • Thyroid Hormone Synthesis • Iodine • Trace element & key component of thyroid hormone • Found in seafood, dairy products, breads, vitamins • Intake of <50 mcg daily leads to hypothyroidism. • Follicles • Site of thyroid hormone synthesis • Spheres of thyroid cells surrounding a colloid core • Inside thyroid cell, iodine is oxidized & bound with tyrosyl residues on thyroglobulin to form thyroid hormone.
The Thyroid (cont’d) • Biosynthesis of thyroid hormone
The Thyroid • Protein Binding of Thyroid Hormone • Two active forms of thyroid hormone: • 1. Triiodothyronine (T3) (3 Iodine) • 2. Tetraiodothyronine (T4) akaThyroxine (4 Iodine) • When released into circulation, only 0.04% of T4 & 0.4% of T3 are unbound by proteins & available for hormonal activity. • Three major binding proteins: • 1. Thyroxine-binding globulin (TBG) • 2. Thyroxine-binding prealbumin (TBPA) • 3. Albumin
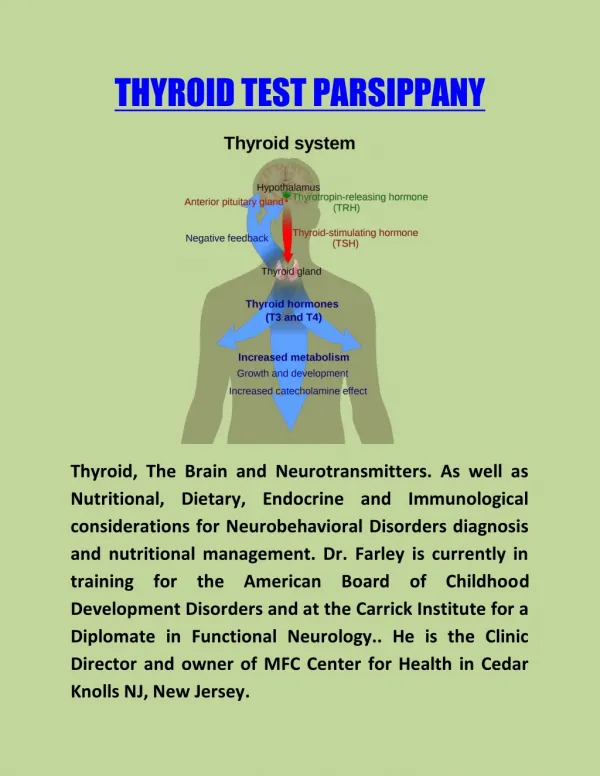
The Thyroid • Control of Thyroid Function • Hypothalamic-pituitary-thyroid axis regulates thyroid hormone production • Thyrotropin-releasing hormone (TRH) – made in hypothalamus • Synthesized by neurons in supraoptic & supraventricular nuclei of hypothalamus • When secreted, stimulates cells in anterior pituitary gland to manufacture & release thyrotropin (TSH) • TSH (made in pituitary) • Circulates to thyroid gland & increases production & release of thyroid hormone (T3 and T4)
The Thyroid (cont’d) • Hypothalamic-pituitary-thyroid axis (Adapted from Surks MI, Sievert R. Drugs and thyroid function. N Engl J Med 1995;333:1688)
The Thyroid • Actions of Thyroid Hormone • Thyroid hormone circulates in bloodstream. • In cytoplasm, T4 is deiodinated into T3 . • T3 leads to proteins that influence metabolism & development. • Effects of thyroid hormone: • Tissue growth • Brain maturation • Increased heat production (thyroid hormones play role in body temp regulation) • Increased oxygen consumption
Thyroid Tests • Blood Tests • TSH (most useful) • 2nd- & 3rd-generation assays used in hormone replacement therapy & to screen for hyper- & hypothyroidism • Serum T4 & T3 • Measured by radioimmunoassay or chemiluminometric assay • Also used to assess/screen for hyper- & hypothyroidism • Thyroglobulin • An ideal tumor marker for thyroid cancer patients • Thyroid autoimmunity • Detects antibodies directed at thyroid tissue
Other Tools for Thyroid Evaluation • Nuclear Medicine Evaluation • Radioactive iodine • Given orally, a % of dose is taken up by thyroid gland. • Assesses metabolic activity of thyroid • Evaluates & treats thyroid cancer • High uptake suggests metabolic activity. • Low uptake suggests metabolic inactivity. • Because TSH stimulates iodine uptake, TSH levels must be taken into account.
Other Tools for Thyroid Evaluation (cont’d) • Thyroid Ultrasound • Has become more significant in past several years • Capable of detecting thyroid nodules of exceptionally small size (<1 cm) • Fine-Needle Aspiration • Often the first step & most accurate tool in evaluation of nodules • Routine use allows prompt identification & treatment of malignancies & avoids unnecessary surgery in benign cases. • Small-gauge needle is inserted into nodule & cells are aspirated.
Disorders of the Thyroid • Hypothyroidism • Low free T4 level with a normal or high TSH • One of most common disorders of thyroid gland, occurring in 5–15% of women >65 years old • Can lead to hyponatremia, anemia, hyperlipidemia • Most common cause in developed countries is chronic lymphocytic thyroiditis (Hashimoto’s Thyroiditis) • Autoimmune disease targeting thyroid gland – enlarged gland or goiter often seen. • Individuals should be tested beginning at age 35 & every 5 years thereafter; more frequently if risk factors are present. • Treated with thyroid hormone replacement therapy • What do you think happens to the body (symptoms) of hypothyroidism? • Weight gain, lethargy/tiredness, cold
Disorders of the Thyroid • Thyrotoxicosis • A constellation of findings that result when peripheral tissues are presented with, & respond to, an excess of thyroid hormone • Possible causes • Excessive thyroid hormone ingestion • Leakage of stored thyroid hormone from thyroid follicles • Excessive thyroid gland production of thyroid hormone (hyperthyroidism) • Symptoms: anxiety, emotional lability, weakness, tremor, palpitations, heat intolerance, perspiration, weight loss – opposite of hypothyroidism
Graves’ Disease • Most common cause of thyrotoxicosis (hyperthyroidism) • An autoimmune disease in which antibodies are produced that activate TSH receptor • Features: thyrotoxicosis, goiter, ophthalmopathy, & dermopathy • Strong familial disposition: 15% of patients have close relative with this condition. • Women are 5 times more likely than men to develop it. • Lab testing shows high free T4 and/or T3 level with undetectable TSH.
Graves’ Disease • Symptoms of ophthalmopathy: orbital soft tissue swelling, injection of conjunctivae, proptosis, double vision, & corneal disease • Treatments • Medication: beta-blockers, propylthiouracil, methimazole • Radioactive iodine: destruction of thyroid tissue to make patient hypothyroid; lifelong treatment with thyroid replacement therapy is usually required • Surgery: preferred in cases of thyroid cancer or to avoid eye problems associated with radioactive iodine treatment
Disorders of the Thyroid • Toxic Adenoma and Multinodular Goiter • Caused by autonomously (independently) functioning thyroid tissue • Neither TSH nor TSH receptor-stimulating immunoglobulin is required to stimulate thyroid hormone production. • Associated with receptor mutations in some toxic nodules • Occur in patients with hyperthyroidism & palpable nodules • Treatment: surgery, radioactive iodine, or medication
Drug-Induced Thyroid Dysfunction • Amiodarone-Induced Thyroid Disease • Amiodarone • Drug ssed to treat cardiac arrhythmias • Fat-soluble with a long half-life (50 days) • 37% of molecular weight is iodine (which accounts for significant part of thyroid dysfunction seen) • Effects • Inhibits thyroid hormone production (Wolff-Chaikoff effect) • Blocks T4 to T3 conversion • Leads to hypothyroidism in 8–20% of patients & hyperthyroidism in 3%
Drug-Induced Thyroid Dysfunction • Subacute Thyroiditis • Characterized by transient changes in thyroid hormone levels • Associated with inflammation of thyroid gland, leakage of stored thyroid hormone, repair of gland • Three classifications • Postpartum: occurs in 3–16% of women in postpartum • Painless: similar to postpartum type, except with no associated pregnancy • Painful: characterized by neck pain, low-grade fever, myalgia, tender diffuse goiter, swings in thyroid function test
Nonthyroidal Illness • Abnormalities in thyroid function tests of hospitalized patients (especially critically ill patients) • Characterized by low total T4, free T4, & TSH • Less T4 is converted to active T3, leading to decreased levels of T3 and higher levels of reverse T3. • Central hypothyroidism & thyroid hormone-binding changes are associated with severe illness. • Changes may be appropriate adaptations to illness. Page 499 - textbook
Thyroid Nodules • Common • Clinically apparent nodules are present in 6.4% of adult women & 1.5% of adult men. • Thyroid ultrasound finds unsuspected nodules in 20–45% of women & 17–25% of men. • 5–9% prove to be thyroid cancer. • Fine-needle aspiration, with cytologic examination of aspirate, is used to determine need for surgical removal. • Page 499 in textbook