Download
1 / 28
280 likes | 452 Views
2. Thyroid Gland. located anteriorly in cervical region, just inferior to thyroid cartilage; two lobes connected by thin isthmus largest purely endocrine gland in body

E N D
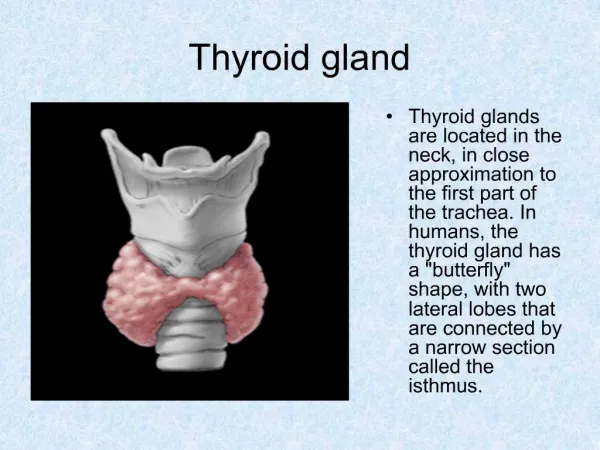
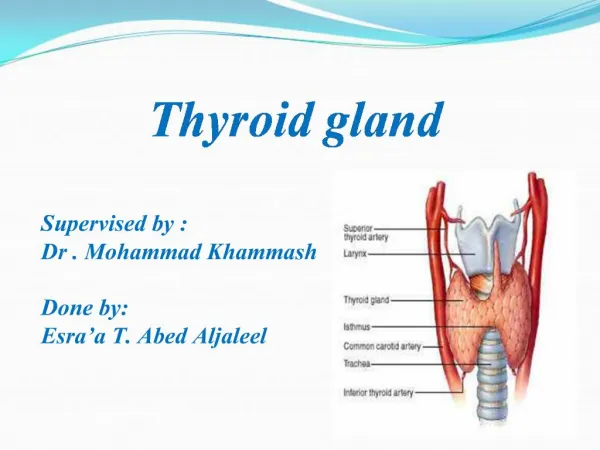
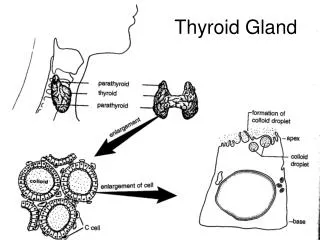
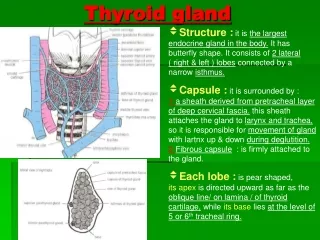
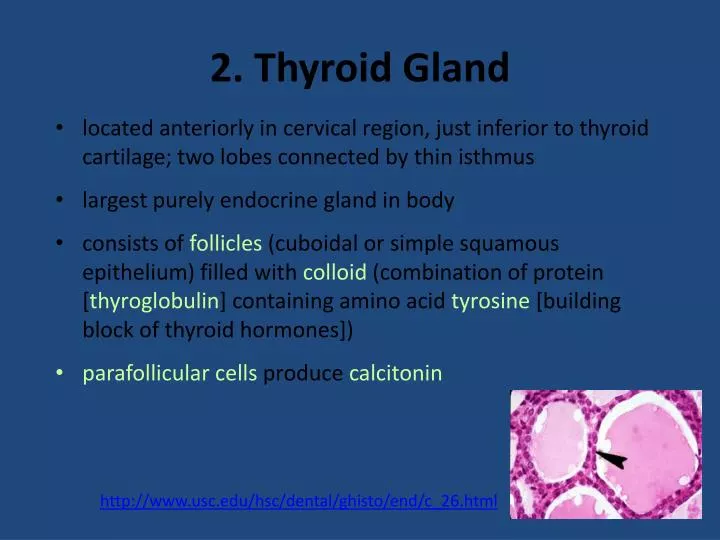
2. Thyroid Gland • located anteriorly in cervical region, just inferior to thyroid cartilage; two lobes connected by thin isthmus • largest purely endocrine gland in body • consists of follicles (cuboidal or simple squamous epithelium) filled with colloid (combination of protein [thyroglobulin] containing amino acid tyrosine [building block of thyroid hormones]) • parafollicular cells produce calcitonin http://www.usc.edu/hsc/dental/ghisto/end/c_26.html
2. Thyroid Gland: T4 and T3 • hormones based on amino acid tyrosine (differ in number of iodine ions) • thyroxine (tetraiodothyronine [T4]) and • triiodothyronine (T3) • T3 is 10x more active, but less common (T4 accounts for about 90% of all thyroid hormone) • much T4 converted to T3 by liver, kidneys, some other tissues
2. Thyroid Gland: T4 and T3 • affect metabolic rate of every cell in the body, except brain, spleen, testes, uterus and thyroid gland • affect other activities within these organs and glands • readily cross membranes (diffuse through plasma membrane to bind to mitochondrial receptors and receptors in nucleus)
T4 and T3: Actions • increase synthesis of enzymes involved in cellular respiration --> increase basal metabolic rate • increases glucose oxidation --> ATP synthesis • increases ATP synthesis in cytoplasm and by mitochondria • results in increased heat production (calorigenic effect) • work with GH to promote normal tissue growth and development, especially important to growth/development of CNS, skeletal and reproductive systems
T4 and T3: Control • release stimulated by TSH (thyroid-stimulating hormone from adenohypophysis) • release of TSH stimulated by TRH from hypothalamus • release of TRH is stimulated by cold, pregnancy, low thyroxine • release inhibited by GHIH, high glucocorticoid levels, high sex hormone levels, high iodine
Hypothyroidism • too little thyroid hormone (thyroid gland defect, inadequate TSH, TRH, or iodine) • Hashimoto’s thyroid– autoimmune disorder in which thyroid is attacked and function decreases • myxedema - low BMR, constipation, puffy eyes, edema, lethargy, mental sluggishness • endemic goiter - enlargement of thyroid gland usually due to lack of sufficient iodine • cretinism - genetic deficiency of thyroid gland or lack of dietary iodine during development resulting in mental retardation, disproportionate growth, short body with thick tongue and neck • treatment - reversed by iodine supplements or hormone replacement therapy
Goiter swelling in neck due to thyroid hypertrophy both hypo- and hyperthyroidism
Hyperthyroidism • too much thyroid hormone (thyrotoxicosis) • Grave’s disease - autoimmune disease in which abnormal antibodies similar to TSH mimic its function and continuously stimulate release of thyroid hormones; results in high BMR, sweating, rapid heart rate, weight loss, restlessness, mood shifts, fatigues easily, limited energy; also toxic goiter • exophthalmos - protrusion of eyeballs, fibrous tissue become edematous (swollen) • treatments - removal of thyroid gland or irradiation • patient must be on synthetic thyroid hormone the rest of his/her life
2. Thyroid Gland: Calcitonin (CT) • polypeptide produced by parafollicular cells • actions: decreases blood calcium levels by: • stimulating osteoblasts (Ca2+ uptake and incorporation into bone) • inhibiting osteoclast activities (osteoclasts break down bone matrix releasing calcium) • control: responds directly to blood calcium levels • very rapid effect • probably more important during childhood when it stimulates bone growth • important because at high blood Ca2+, membranes become less permeable to Na+
3. Parathyroid Glands • 2 paired structures on posterior of thyroid gland • oxyphyil cells - function unknown • chief cells secrete parathyroid hormone (PTH; protein) • actions: increases blood Ca2+ by: • stimulating osteoclast activity (which break down bone matrix) while inhibiting osteoblasts (which form bone matrix) • stimulating increased reabsorption of Ca2+ by kidney • indirectly stimulating increased absorption of Ca2+ by small intestine by causing secretion of calcitrol form kidneys
3. Parathyroid Glands http://www.usc.edu/hsc/dental/ghisto/end/c_32.html
Hyperparathyroidism • rare; caused by parathyroid gland tumor • results in hypercalcemia (excess Ca2+ levels in blood) --> depression of nervous system (because of effect on sodium permeability), abnormal reflexes, skeletal muscle weakness, nausea, vomiting, kidney stones, calcium deposits in soft tissues; bones become soft
Hypoparathyroidism • trauma to or removal of parathyroid gland • results in hypocalcemia (low blood Ca2+) --> neurons become too excitable --> muscle tetany --> spasms/cramps --> respiratory paralysis --> death
4. Adrenal Glands • located in abdominal cavity against back wall (retroperitoneal), superior to kidney • surrounded by connective tissue capsule • two regions: • cortex - outer region, “glandular”, three zones • zona glomerulosa - outer zone • zona fasciculata - middle zone • zona reticularis - inner zone • medulla - inner region, modified neural tissue (develops from same tissue in embryo as ganglionic [postganglionic] neurons of sympathetic division)
Adrenal Cortex: Zona Glomerulosa • produces steroid hormones based on cholesterol • mineralocorticoids - ion (and water) balance • main hormone is aldosterone • action: • stimulates reabsorption of Na+ and secretion of K+ from kidney, sweat glands, salivary glands, pancreas • secondarily, increases water reabsorption in kidney (water follows Na+)
Adrenal Cortex: Zona Glomerulosa control: • aldosterone release stimulated by: • high K+, low Na+ • angiotensin II (result of renin-angiotensin pathway stimulated by low blood pressure), • ACTH (when under severe stress) • inhibited by low K+, high Na+
Adrenal Cortex: Zona Glomerulosa Disorders: • aldosteronism = hypersecretion (adrenal tumor) • increased water and Na+ reabsorption --> hypertension, edema; • loss of K+ --> disruption of neural and muscle function
Adrenal Cortex: Zona Glomerulosa Disorders: • Addison’s Disease = hyposecretion glucocorticoids and mineralocorticoids • results in decreased Na+ and water reabsorption, increased blood K+ --> low blood volume --> hypotension, dehydration; • changes in membrane potentials --> disruption in neural and muscular function • also decreased cortisol secretion by zona fasciculata --> decreased blood glucose levels (especially during prolonged stress)
Adrenal Cortex: Zona Fasciculata • glucocorticoids - effects on glucose metabolism • main hormone is cortisol (hydrocortisone) • actions: • maintains blood glucose levels, especially in times of stress, by: • promoting gluconeogenesis (making new glucose in liver) and use of alternative fuels by other cells (saves glucose for the brain) • anti-inflammatory decrease immune response • can be used clinically to treat allergic reactions (e.g., poison ivy), rheumatoid arthritis
Adrenal Cortex: Zona Fasciculata • Control • stimulated by ACTH • inhibited by cortisol (inhibits secretion of CRH from hypothalamus) • blood levels peak in the morning Disorders: • Addison’s Disease - hyposecretion of glucocorticoids and mineralocorticoids
ZonaFasciculata: Cushing’s Disease • hypersecretion of glucocorticoids • caused by hypersecretion of ACTH due to tumor in ZF, pituitary, lungs, kidneys, or pancreas • suppresses glucose metabolism resulting in • hyperglycemia (elevated glucose= steroid diabetes), • stimulates lipid metabolism (weight loss), • loss of muscle and bone mass, • “buffalo neck” and “moon face” (fat redistribution), • anti-inflammatory effects (mask infection) • water and salt retention (effect of aldosterone hypersecretion --> water retention --> hypertension)
Adrenal Cortex: Zona Reticularis • gonadocorticoids • most are androgens (“male” sex hormones) - converted to testosterone; small amounts of estrogens • actions: may contribute to onset of puberty (levels rise between 7 and 13 years of age; exact function compared to hormones from ovaries or testes unclear) • control: stimulated by ACTH
Adrenal Cortex: Zona Reticularis • hypersecretion results in: • masculinization and masculine pattern of hair distribution in females • in males - rapid maturation of reproductive organs, secondary sex characteristics; hypersecretion of estrogens causes feminization and gynecomastia (enlarged breasts)
Adrenal Medulla • chromaffin cells (modified neurons - arise from same embryonic tissue as postganglionic neurons of sympathetic division) • catecholamines - epinephrine (~80%), norepi (NE) • control: secretion stimulated by preganglionic fibers of sympathetic nerves during flight-or-fight response
Adrenal Medulla • actions: • epinephrine (more potent) - increases HR (beta receptors), bronchodilation (in lungs), increased blood glucose (breakdown of glycogen in liver and skeletal muscle, and breakdown of adipose tissue) • NE - peripheral vasoconstriction --> increased BP