Download
1 / 25
250 likes | 310 Views
Caesarean section. an operative procedure, which is carried out under anesthesia (regional or general), whereby the fetus, placenta and membranes are delivered through an incision made in the abdominal wall and uterus.

E N D
Caesarean section • an operative procedure, which is carried out under anesthesia (regional or general), whereby the fetus, placenta and membranes are delivered through an incision made in the abdominal wall and uterus. • clinical characteristics of the population, such as maternal age, ethnicity, previous CS, breech presentation, prematurity and induction of labour.
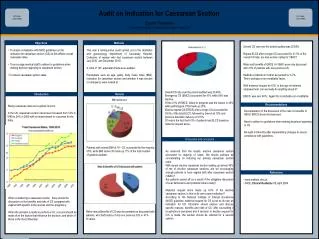
a primary CS were: • failure to progress in labour • fetal compromise • breech presentation • previous CS • maternal request • complications during labour that provide an indication for CS. • (e.g. eclampsia, abruptio placenta)
the indications for caesarean section • Immediate threat to the life of the woman or fetus. • Maternal or fetal compromise which is not immediately life-threatening. • No maternal or fetal compromise but needs early delivery. • Delivery timed
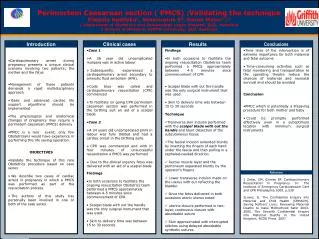
in utero fetal resuscitation (fluids, tocolytics and oxygen) may give enough time for a more considered and careful approach.
elective caesarean section : • Past obstetric history • previous classical caesarean section • interval pelvic floor or anal sphincter repair(rectocele ) • previous severe shoulder dystocia with significant neonatal injury.
Current pregnancy events • significant fetal disease • monoamniotic twins or higher-order multiple pregnancy • placenta praevia • obstructing pelvic mass • active primary herpes at onset of labour
Intrapartum events • fetal compromise in the first stage • maternal disease • cephalopelvic disproportion (brow presentations etc).
The operative procedure • The procedure is explained and consent obtained (written consent)A preoperative assessment includes: weight , blood pressure, pulse and temperature. • gowned, make-up, the presence of any nail varnish and jewellery removed (rings/ear-rings taped).
anaesthetic chart. • blood tests (full blood count, group and save and cross match. • antacid therapy. • urinary catheterization
lie flat, it is essential that a wedge or cushion is used supine hypotension ), • The regional or general anesthesia. • The skin is prepared • Intravenous antibiotics should be administered as surgical prophylaxis before the skin is incised.
. • The anatomical layers to reach the fetus are: skin, subcutaneous fat, rectus sheath, muscle (rectus abdominis), abdominal peritoneum, pelvic peritoneum and uterine muscle.
A transverse lower abdominal incision (bikini line incision) is usually performed with the skin and subcutaneous tissues incised using a transverse curvilinear incision at a level of two fingerbreadths above the symphysis pubis. • The subcutaneous tissues are subsequently separated by blunt dissection and the rectus sheath incised transversely for 2 cm either side of the midline.
This incision is then extended with scissors or blunt dissection before the facial sheath is separated from the underlying muscle. • The recti are separated from each other • the peritoneum incised and the abdominal cavity entered.
-The fold of the peritoneum over the anterior aspect of the lower uterine segment and above the bladder is incised and the bladder mobilized and reflected down. • The uterus is incised transversely taking care not to cause surgical trauma to the fetus (a significant risk in the presence of low levels of amniotic fluid). • The surgeon, with help from the surgical assistant (who must apply fundal pressure), will then secure the safe delivery of the baby.
-The main reason for preferring the lower uterine segment technique is the reduced incidence of dehiscence of the uterine scar in any subsequent pregnancy and/or birth when compared to a classical or vertical incision (which may be the only surgical approach that is suitable in situations such as anterior wall placenta praevia, in extreme prematurity (where no lower uterine segment may be formed) or in the presence of dense adhesions from previous surgery.
-Oxytocics (a bolus of 5 IU of Syntocinon) should be given by the anaesthetist after birth of the baby and clamping of the umbilical cord. • -When the baby and placenta have been delivered, the uterus is closed in two layers and the rectus sheath and skin sutured. • Most surgeons use a braided polyglactin suture (Vicryl) for all layers. • The wound is then dressed and the vagina swabbed to remove any clots. • This also allows a final intraoperative assessment of any ongoing bleeding from within the uterus.
-Women having a CS should be offered thromboprophylaxis because they are at increased risk of venous thromboembolism • stockings, hydration, early mobilization, low molecular weight heparin) should take into account risk of thromboembolic disease,
administer low molecular weight heparin to all women until they are fully mobile. Those with an increased risk (e.g. maternal obesity or concurrent maternal morbidity)
-Early skin-to-skin contact between the woman and her baby should be encouraged and facilitated as it : • improves maternal perceptions of the infant, mothering skills, maternal behaviour, breastfeeding outcomes and reduces infant crying • -CS should be offered additional support to help them to start breastfeeding as soon as possible after the birth of their baby.
-caesarean section are less likely to start breastfeeding in the first few hours after the birth, but, when breastfeeding is established, they are as likely to continue as women who have had a vaginal birth.
Women's request for caesarean section • very few women actually request CS in the absence of medical indications • women who have had difficult experiences of childbirth
Psychological support and the role of the midwife • -Women actively involved in their care and all staff involved must ensure that recent, valid and relevant information is provided in a comprehensible manner.
One-to-one care from a support person during labour can influence the rate of birth by CS benefit, both to the woman and to her family ,It is important that midwives recognize the positive impact • Psychological support also help these women to overcome their fears ,their anxieties