Download
1 / 1
10 likes | 120 Views
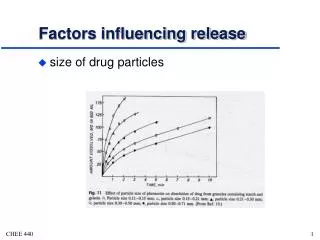
Factors influencing caesarean section infection rates B Karunakaran, R Oakes, N Biswas, N McCord Poole Hospital Foundation NHS Trust, Dorset, UK. Introduction. Methods. Results. Conclusions.

E N D
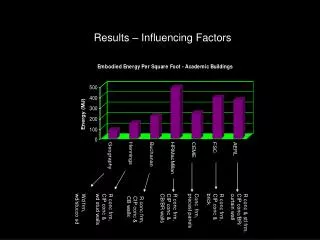
Factors influencing caesarean section infection rates B Karunakaran, R Oakes, N Biswas, N McCordPoole Hospital Foundation NHS Trust, Dorset, UK Introduction Methods Results Conclusions Post caesarean section surgical site infection (SSI) is a major problem in Obstetrics, contributing to maternal morbidity,negatively impacting on patient experience and incurring significant cost to the NHS. The caesarean section infection rate varies depending on source. Internationally, rates ranging between 2.0% and 25% have been reportedthink. Poole Hospital is a secondary care provider with annual delivery rate of over 4,000 births per annum. The surgical site infection rate following Caesarean section between 2010-11 was 16%. This study was part of an initiative which aimed to investigate and identify the variable factors thatinfluence the caesarean section infection rate. • This was a retrospective case control study. Patient cases were selected from a three month period between May and June 2010. • All cases of infection were identified and reviewed. A selection of non-infected cases were also reviewed. • Cases were identified from clinical coding. For the purpose of the study patients with surgical siteinfection were defined as those who presented following theircaesarean section to a healthcare professional and were clinicallydiagnosed as having a SSI. • Data was collected on a 46 different variables in broadly four different categories. These included: • Patient Demographics • Surgical factors • Anaesthetic factors • Labour and post natal • 326 Caesarean sections were performed over the study period. 137 case notes were reviewed. There were 42 cases of infection. Forest plot demonstrating associations between SSI and variables investigated in our study We found a statistically significant association between highBMI and SSIs, with an odds ratio of 4.9 (95% CI 2.13 to 11.2) There was also an association between smoking and SSIs, with an oddsratio of 2.31 approaching significance (95% CI of 0.96 to 5.6). Afurther association between those patients who had manual removal ofplacenta (MROP) and SSIs, with an odds ratio of 3.99 approachingsignificance (95% CI of 0.91 to 17.54). No significant association wasestablished between steroids in labour, previous caesarean sections,emergency vs. elective caesarean sections, estimated blood loss or theseniority of the surgeon operating. This study supports previous literature reporting a significant association betweenhigh BMI and SSIs. We recommend further emphasis on weight reduction for women planning pregnancies to reduce the risk of SSIs. We suggest that further research into the possible changes to wound care for women with high BMI to reduce the risk of SSIs. As our study is suggestive of some association between MROP and SSIs, a largerstudy is warranted to establish this relationship and the impact of giving a prolonged course ofantibiotics following MROP in Caesarean section (as routinely done inpatients who have MROP per vaginum.) Overallthe association between modifiable factors and post Caesarean SSI ispromising for future scope of reducing infection rate and improvingpatient outcome. Beattie P, Rings T, Hunter M et al. (1994) Risk factors for wound infection following caesarean section. Aust NZ J Obstet Gynaecol. 34:298±302. Wilson J (1995) Infection Control in Clinical Practice. Bailliere Tindall, London. Opøien HK, Valbø A, Grinde-Anderson A, Walberg M. Post-cesarean surgical site infections according to CDC standards: rates and risk factors. A prospective cohort study. Acta Obstet Gynecol Scand. 2007;86(9):1097-102. References