Download
1 / 22
220 likes | 363 Views
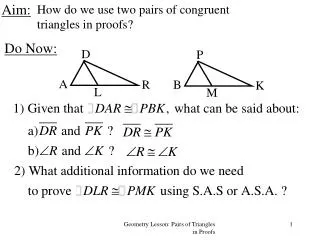
Aim. To provide information about Mersey Care’s Complaints Process and Adverse Incidents Policy & procedures. Objectives. Give an overview of the current complaints Process Define what is an adverse incident Identify your responsibilities in reporting an adverse incident

E N D
Aim To provide information about Mersey Care’s Complaints Process and Adverse Incidents Policy & procedures
Objectives • Give an overview of the current complaints Process • Define what is an adverse incident • Identify your responsibilities in reporting an adverse incident • Importance of learning from Complaints / Incidents
Making Experiences Count • New process introduced by Department of Health in April 09 • Main Objectives • Removal of prescriptive timescales • Involve complainant from the outset • Respond to majority of complaints quickly • Consider all possible methods of finding a resolution • Ensure all NHS agencies and Social Care organisations work together to provide a single response to the complainant • A more outcome driven process
Local Resolution • Initially staff should try and help resolve the issue locally • Involve PAL’s if appropriate • If they are still not happy provide information to contact Complaints Department
Complainant contacts complaints department • Complaints Department liaises with the complainant with the aim of: • Confirming the nature of complaint • Discussing desired outcomes • Agree possible method of resolution
Complainant contacts complaints department • Complaints Department will contact CBU or Department • Agree the route to achieve resolution for the complainant Examples are; • Set up meeting with complainant and those involved in delivery or managing the care. • Complaint investigation • Independent review • Conciliation
Right to Appeal Complainant has the right to refer to the Parliamentary and Health Service Ombudsman
Viewing complaints positively • Complaints are often viewed negatively. They do however play a vital part in continuous service improvements • Complaints can be stressful for staff involved and the department aim to support all staff by: • Notifying staff of complaints they have been involved in via their line manager • Provide an explanation of what will happen during the process and who is available for support via their line manager • Ensuring feedback is provided individually to staff involved • Complaints are not investigated in order to apportion blame
What is an Adverse Incident? Any event or circumstance that could have or did lead to unintended or unexpected harm, loss or damage relating to service users, members of staff, the public or trust property
An Organisation with a Memory Report of Expert Group on Adverse Events in the NHS • 400 people die or are seriously injured by medical devices • 1,150 people who've been in recent contact with mental health services commit suicide • 10,000 people have serious adverse reaction to prescribed drugs • 28,000 written complaints are made about clinical treatment in hospitals • £400m paid out by NHS to settle negligence claims now risen to £710m • £1 billion cost to NHS from hospital acquired infections. Type of infections have changed
An Organisation with a Memory Report of Expert Group on Adverse Events in the NHS The same kinds of very serious adverse events happen time and again, year after year Enquiries are held ‘lessons must be learned’ But they are not!
Failures • Why Do Things Go Wrong? • Active failures – ‘unsafe acts’ • Latent conditions – lying dormant before combining with ‘unsafe acts’ to cause an Adverse Event
Custom and Practice • Most people pick up some ‘bad rules’ (bad habits) when learning a job. • They are ‘bad’ because they can lead to something going wrong at a later time, even though they might serve their immediate purpose on many occasions. • Such ‘bad rules’ become established as part of the person’s ‘tool bag’. • We normalise the abnormal • We do not challenge this
Failing to apply good rules • Violations increase the chances of subsequent error(s) having bad consequences
Poor Procedures In the nuclear power industry, 67% of all human performance problems have been traced to bad (incorrect, absent or unworkable) procedures.
Why don’t people report • Too busy • Too difficult • Forms disappear into a black hole • Nothing ever changes • Frightened of negative outcomes
Why should they report • Forms are read and acted upon • All forms are read at least twice. • 11000 forms a year • A way of learning • Can help make an area safe • Can improve both individual and team practice • Monitor for trends
Cartoon An Organisation with a Memory Report of expert group on Adverse Events in the NHS
THE WAY FORWARD • Unified Mechanism for Reporting & Analysis when things go wrong
Root Cause Analysis • "Root Cause Analysis is a methodology that enables you to ask the questions • 'What', • ‘How' and • ‘Why' in a structured and objective way to reveal all factors that have led to a patient safety incident" “NPSA e-learning programme”
Root Cause Analysis • The process involves: • Defining the problem and its actual or potential effects. • Determining what exactly happened. • Determining how this varied from what should have happened. • Determining why it happened (the root and contributory causes). • Developing corrective actions that would prevent reoccurrence.
Contact Numbers • Steve Morgan 0151 473 2873 • Adverse Incident Support 0151 473 2877 • Emma Howell Security Management Service 0151 471 2305 • Dave Hurley Datix System Manager 0151 472 4543 • Liz Williams Complaints Lead Local Services 0151 471 2645 • Scott Yates Complaints Lead High Secure and Forensic 0151 471 2219