Download
1 / 8
80 likes | 258 Views
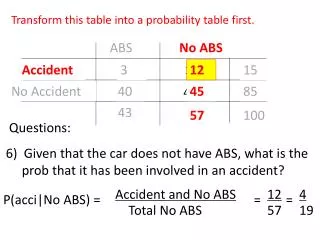
1 of 2. Frequency of Clostridium difficile infection (CDI) transmission via ward contact with a known case. Retrospective, observational study (22 months; 1 laboratory providing diagnostic services for all inpatient and community care in Leeds, UK)

E N D
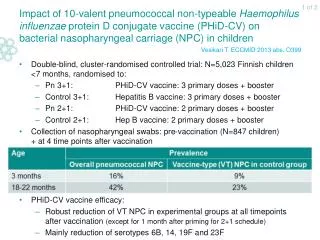
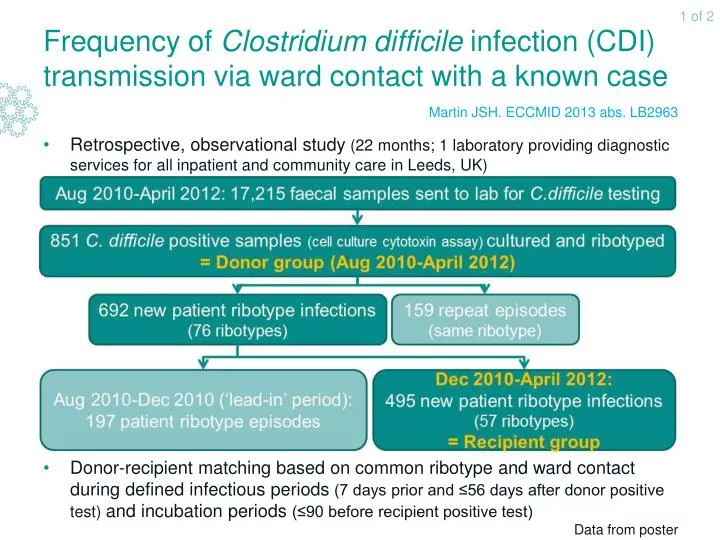
1 of 2 Frequency of Clostridium difficile infection (CDI) transmission via ward contact with a known case Retrospective, observational study (22 months; 1 laboratory providing diagnostic services for all inpatient and community care in Leeds, UK) Donor-recipient matching based on common ribotype and ward contact during defined infectious periods (7 days prior and ≤56 days after donor positive test) and incubation periods (≤90 before recipient positive test) Martin JSH. ECCMID 2013 abs. LB2963 Data from poster
2 of 2 Frequency of Clostridium difficile infection (CDI) transmission via ward contact with a known case • Inpatient samples: Donor group: 75% - Recipient group: 78% Martin JSH. ECCMID 2013 abs. LB2963 Data from poster
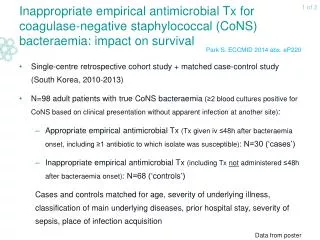
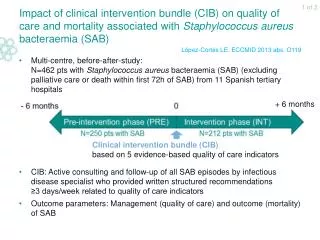
1 of 2 Impact of new liquid oxygen releaser surface disinfectant on risk of nosocomial Clostridium difficile infection (CDI) Single-centre before-after study (2 wards of internal medicine department of university hospital; Austria): Pre-intervention phase: Conventional sporocidal surface disinfection; used only in response to occurrence of nosocomial CDI Intervention phase: New liquid oxygen releaser disinfectant; used daily, regardless of CDI occurrence Hell M. ECCMID 2013 abs. O448
2 of 2 Impact of new liquid oxygen releaser surface disinfectant on risk of nosocomial Clostridium difficile infection (CDI) Daily use of a liquid oxygen releaser disinfectant may significantly reduce the incidence of nosocomial CDI compared with conventional disinfection Hell M. ECCMID 2013 abs. O448
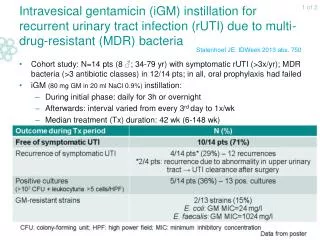
1 of 2 Effectiveness of donor faeces infusion for treating recurrent Clostridium difficile infection (CDI) Single-centre randomised controlled trial (2008-2010): N= 42 pts with recurrent CDI: Group 1 (N=16): Initial vancomycin (500 mg orally 4x/day for 4 days) + bowel lavage + duodenal infusion of donor faeces through nasoduodenal tube (+ 2nd infusion with donor faeces of different donor if no resolution of diarrhoea after 1st infusion) Group 2 (N=13): Standard vancomycin regimen (500 mg orally 4x/d for 14 d) Group 3 (N=13): Standard vancomycin regimen (500 mg orally 4x/d for 14 d) + bowel lavage Primary endpoint: Resolution of diarrhoea without relapse after 10 wk Study was stopped after interim efficacy analysis No sign. ≠ in baseline characteristics between treatment groups van Nood E et al. N Engl J Med 2013;368:407-15
2 of 2 Effectiveness of donor faeces infusion for treating recurrent Clostridium difficile infection (CDI) van Nood E et al. N Engl J Med 2013;368:407-15
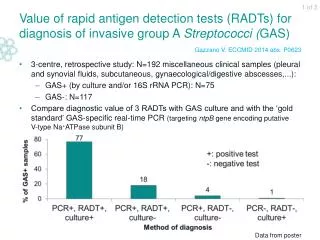
1 of 2 Efficacy and safety of fidaxomicin vs vancomycin for Clostridium difficile infection: phase III non-inferiority trial Multi-centre, double-blind, randomised, non-inferiority trial (Europe, USA, Canada; 2007-2009) N= 535 pts with acute, toxin-positive C.difficile infection (CDI): Fidaxomicin (FDX) (N=270): 200 mg orally every 12h for 10 days Vancomycin (VCA)(N=265): 125 mg orally every 6h for 10 days 26 pts excluded; 509 pts included in modified intention-to-treat (mITT) population Safety(safety population: N=524)No significant differences in TEAEs between treatment groups Cornely OA et al. Lancet Infect Dis 2012;12:281-9 TEAE: treatment-emergent adverse event; * Possibly or definitely related to study drug
2 of 2 Efficacy and safety of fidaxomicin vs vancomycin for Clostridium difficile infection: phase III non-inferiority trial Efficacy • Primary endpoint: Clinical cure = resolution of diarrhoea and no further need for treatment • Tested hypothesis: FDX is non-inferior to VCA for primary endpoint;Criterion for non-inferiority: 1-sided lower 97.5% CI margin: -10% • Subgroup analyses of primary endpoint in mITT population: no sign. ≠Except: Fidaxomicin seems to be non-inferior to vancomycin for initial clinical response to CDI and seems to have a comparable safety profile Cornely OA et al. Lancet Infect Dis 2012;12:281-9