Download

1 / 40
500 likes | 1.19k Views
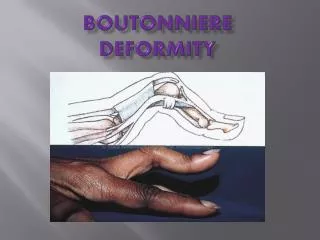
Swan Neck Deformity. Swan neck deformity. The volar plate is torn, causing the joint to open abnormally under the pull of the extensor ligaments. Swan-Neck Deformity. Typically defined as: proximal interphalangeal (PIP) joint hyperextension

E N D
Swan neck deformity. The volar plate is torn, causing the joint to open abnormally under the pull of the extensor ligaments.
Swan-Neck Deformity • Typically defined as: • proximal interphalangeal (PIP) joint hyperextension • with concurrent distal interphalangeal (DIP) joint flexion • Not necessarily unique to RA but rather an end result of muscle and tendon imbalance caused by RA.
Swan-Neck Deformity • Not necessarily unique to RA but rather an end result of muscle and tendon imbalance caused by RA
Nalebuff Classification1989 • Type I - PIP joints flexible in all positions • No intrinsic tightness or functional loss • Type II - PIP joint flexion limited in certain positions • Intrinsic tightness • Limited PIP motion with extended MCP with ulnar deviation • Type III - PIP joint flexion limited in all positions • Near normal radiograph • Type IV - PIP joints stiff with poor radiographic appearance
Pathophysiology • The intercalated joint collapse concept of Landsmeer means that collapse of a joint in one direction will result in deformity of the next distal joint in the opposite direction. • Z deformity
Pathophysiology • In a normal finger, intrinsic muscles serve as: • flexors of the MCP joint • extensors of the PIP and DIP joints • By being located volar to the MCP joint axis and dorsal to the PIP and DIP joint axes
Pathophysiology • Intrinsic tightness increases the flexor pull on the MCP joint and hyperextension of PIPJ • Weak flexor power aggravates this by being unable to pull the middle phalanx. • DIPJ and MCPJ hyperextension follows • Constant efforts to extend the finger against this pull then leads to stretching of the collateral ligaments and weakening of the volar plate at the PIPJ.
Pathophysiology • the lateral bands are constrained in their dorsal position with the extensor apparatus migrating proximally • therefore upsetting the flexor-extensor balance, • The lateral bands in this position act to increase the pull of the central slip that attaches to the dorsal base of the middle phalanx. • Leading to hyperextension of PIPJ
Pathophysiology • The increase of FPL tension resulting from hyperextension of the PIP joint leads to a reciprocal flexion of the DIP joint. • DIP mallet deformity also from: • Joint erosion • Extensor tendon attentuation or rupture • Progressive disease leads to joint destruction and fixed contracture.
Hashemi-Nejad and Goddard (1994) -multidisciplinary approach is best -an affected joint will affect other joints -early synovectomy is worthwhile after a 6-month trial of non-operative treatment -tenosynovectomy decreases the risk of tendon rupture, -the wrist is the key in the RA hand -the thumb is a very important source of disability -silastic MCPJ arthroplasty is successful in reducing pain and improving function
Feldon (1993) lists the aims of surgery in the RA hand: 1. pain relief 2. functional improvement 3. preventing disease progression 4. cosmetic improvement Note that the presence of a painless deformity with minimal function deficit is not an indication for surgery.
Management • Millender and Nalebuff staging system (1975) is a good guideline for identifying treatment options in RA
Principles • Prevention • Correct PIPJ hyperextension • Restore DIPJ extension
Type1 • Silver ring splint to flex PIPJ • Volar dermatodesis • Correction of any MCPJ abnormality first • Flexor tenosynovectomy (if synovitis is present) • Flexor tenodesis - FDS slip through A2 pulley then looped back to itself • Retinacular ligament reconstruction • Release ulnar lateral band proximally and pass volar to PIPJ axis sheath
Permit active PIP flexion and limit hyperextension of the PIP joint Silver Ring Splint
DIP Fusion • Difficult and unreliable to restore the extensor apparatus at DIP level cause underlying RA disease will destroy the repair • Also secondary arthritis within DIP may make attempts to mobilise joint unwise
Dermadesis • Used to prevent PIP hyperextension bu creating a skin shortage volarly • Elliptical skin wedge (4-5mm at widest) is removed from volar aspect of PIP • Care not too disturb venous drainage or violate the flexor sheath • Skin closed with PIP in flexion • Only useful if done in conjunction with other procedures ie DIP fusion
Flexor Tendon Tenodesis“sublimis sling” • Used as checkrein against hyperextension ie restoration of strong volar support • One slip of FDS is divided ~1.5cm proximal to PIP • This is then separated from its corresponding slip bit left attached distally • With joint at 20-30 degrees the detached slip is fixed proximally • Anchored to thickened margin of sheath, distal edge of A2 or Mitek • Nalebuff did simpler procedure whereby he passed split tendon around A1 pulley
Reticular Ligament Reconstruction • Credited to Littler • Ulnar lateral band is freed from extensor mechanism proximally but left attached distally • Passed volar to Cleland’s fibres to bring it volar to axis of PIP • Band is sutured to the fibrous tendon sheath under enough tension to restore DIP extension and prevent hyperextension at PIP • However, in RA may have destruction of terminal tendon so no amount of tension applied to the relocated tendon will achieve DIP extension
Type 2 • Looks like Type 1 but PIP movement is limited in certain positions related to position of MCPJ • MCPJ extended/radial deviation then limited passive PIP ROM • MCPJ flexed/ulnar deviated then PIP ROM increased • As MCPJ subluxates and the intrinsics get tight a secondary swan neck develops as a result of muscular imbalance • Not sufficient to restrict PIPJ hyperextension, intrinsics must be released plus MCPJ subluxation must be corrected +/- arthroplasty
Intrinsic Release • Photo on camera • A rhomboid portion of the ulnar extensor aponeurosis is then resected • This procedure resects the lateral band through which the abnormally tight intrinsics have caused MP flexion and PIP hyperextension
Type 3 • unlike type 1 & 2 have significant functional disability due to inability to grasp objects • Not joint destruction but restriction due to: • Extensor mechanism • Collateral ligaments • Skin • First goal is to restore passive ROM • PIPJ manipulation • Skin release • Lateral band mobilisation • Then correction of deformity after motion restored
PIPJ Manipulation • MUA possible up to 80-90 degrees • Usually in conjunction with intrinsic release, arthroplasty or tenosynovectomy
Skin Release • Dorsal skin may limit the amount of passive flexion that is achieved during manipulation • Tension minimised with an oblique incision just distal to the PIPJ • Allowing skin edges to spread • Closes 2-3 weeks by secondary intention • PHOTO 2112
Lateral Band Mobilisation • Lateral bands are displaced dorsally • Free lateral bands from central slip using 2 parallel incisions allows flexion without releasing lateral bands or lengthening central slip • PHOTO 2113
Type 4 • Patients with stiff PIPJ and radiographic evidence of advanced intra-articular changes require salvage procedure • Fusion or arthroplasty • PHOTO 2114