Download
1 / 33
330 likes | 522 Views
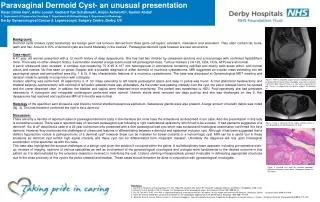
Case presentation- an enteric cyst . Patient’s profile. Name: 張 o 幃 Chart No.: 12577023 Age: 27 Gender: Female Occupation: 商 Date of admission: 2009. 1. 3 Date of operation: 2009. 1. 4 Date of discharge: 2009. 1. 9. Chief complaint.

E N D
Patient’s profile • Name:張o幃 • Chart No.:12577023 • Age: 27 • Gender: Female • Occupation: 商 • Date of admission: 2009. 1. 3 • Date of operation: 2009. 1. 4 • Date of discharge: 2009. 1. 9
Chief complaint • Asymptomatic mass in anterior mediastinum noted for about 2 months
Present illness • This 27 y/o female has medical history of right breast fibroadenoma s/p excision about nine months ago (98/3) at Holy Cross Hospital in America. • She accepted general health examination last October. Mediastinal widening was noted over chest X ray.
Present illness • There was no symptom including cough, dyspnea, hemoptysis, orthopnea, PND, body weight loss, poor appetite, night sweating or fever. • Chest CT showed a solid anterior mediastinal tumor with septum. Ga 67 scan showed no evidence of gallium-avid tumor. CT guided biopsy was performed on 12/17.. • This time she is admitted for tumor excision.
Past and personal history • Diabetes Mellitus, Hypertension:denied • Cardiovascular disease, Cerebrovascular accident: denied • Asthma, ESRD: denied • Other systemic disease: bilateral fibroadenoma at 98/3 in Holy Cross Hospital of America • Operation history: denied • Alcohol, Betal nuts, Cigarette smoking: denied • Contact history: denied • Travel history: no recent travel history • Allergy history: NKFDA • Family history: no contributory
Physical examination • Consiousness: alert GCS: E4V5M6 • BP: 117 / 69 mmHg, PR: 70 bpm, RR: 18 cpm, BT: 36.6℃ • Conjunctiva: not pale Sclera: no icteric • Neck: supple,lymphoadenopathy(-), jugular vein engorgement(-) • Chest: symmetric expansion, no deformity • bilateral clear but breath sound • Heart sound: regular heart beat,no murmur, S3(-), S4(-) • Abdomen: mild obesity, soft and flat, tympanic • Bowel sound: normooactive • Palpation: No rebounding pain, no muscle guarding, no flank knocking pain, Murphy sign (-), caput medusa (-), spider angioma (-), Liver/Spleen: impalpable • Extremities: freely movable, no pitting edema
Tentative diagnosis • A solid anterior mediastinum tumor, suspect teratoma
Plans • Arranged VATS excision tomorrow • Pre- operational preparation
OP finding Tumor (medial) Collapsed lung (lateral)
OP finding Tumor Pericardium
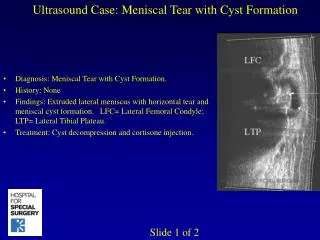
Pathology diagnosis • Enteric cyst. • GROSS FINDING: • tumorous mass attached with thymus and pericardium • measuring 10x6x5 cm and weighing 150 gm. • multilocular mass filled with greenish, sticky content. • MICROSCOPIC FINDING: • mutilocular cystic mass composed of intetinal mucosa and associated muscle layer admixed with adipose tissue, nerve bundles are ganglia.
Usual location of the common primary tumors and cysts of the mediastinum
Character of mediastinum tumor • approximately 25% of mediastinal tumors are malignant. • two thirds of mediastinal tumors in adults are discovered as asymptomatic abnormalities on radiologic studies • Characteristics such as size, location, rate of growth, and associated inflammation are important factors that correlate with symptoms.
Enteric cyst • posterior division of the primitive foregut • frequently located in the posterior mediastinum • composed of smooth muscle with an inner epithelial lining of esophageal, gastric, or intestinal mucosa • peptic ulceration with perforation into the esophageal or bronchial lumina may occur • enteric cysts have an attachment to the esophagus and may be embedded within the muscularis layer
Accepted mediastinal indication for VATS • Biopsy of mediastinal lymph nodes • Biopsy of mediastinal masses • Resection of benign germ cell tumors • Resection of ectopic parathyroid • Resection of thymus for thymic cyst, myasthenia gravis, stage I thymoma • Resection of bronchogenic or pericardial cysts • Esophageal cystectomy
Accepted mediastinal indication for VATS • Enucleation of esophageal leiomyomas • Esophagomyotomy for achalasia • Resection of posterior mediastinal (neurogenic) tumors • Thoracic dorsal sympathectomy for palmar and axillary hyperhidrosis • Thoracic splanchnicectomy for chronic intractable abdominal pain
REFERENCE • Intern Med. 2007;46(11):781-4. Epub 2007 Jun 1. • Schwart’s principle of surgery, 9th • Sabiston, 18th