Download
1 / 1
10 likes | 399 Views
Paravaginal Dermoid Cyst- an unusual presentation Hsiao Chien Gan 1 , Ashu Loona 2 , Gerhard Van Schalkwyk 2 , Alison Ashworth 3 , Summi Abdul 1 1. Department of Gynaecoloy Oncology 2. Department of Histopathology 3. Department of Radiology

E N D
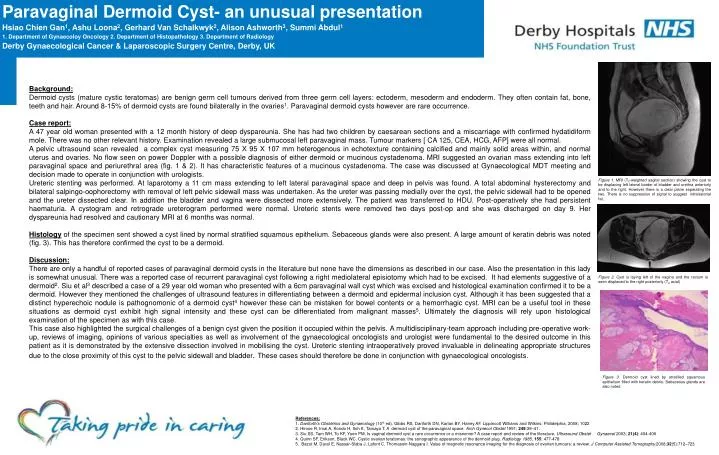
Paravaginal Dermoid Cyst- an unusual presentation Hsiao Chien Gan1, Ashu Loona2, Gerhard Van Schalkwyk2, Alison Ashworth3, Summi Abdul1 1. Department of Gynaecoloy Oncology 2. Department of Histopathology 3. Department of Radiology Derby Gynaecological Cancer & Laparoscopic Surgery Centre, Derby, UK Background: Dermoid cysts (mature cystic teratomas) are benign germ cell tumours derived from three germ cell layers: ectoderm, mesoderm and endoderm. They often contain fat, bone, teeth and hair. Around 8-15% of dermoid cysts are found bilaterally in the ovaries1. Paravaginal dermoid cysts however are rare occurrence. Case report: A 47 year old woman presented with a 12 month history of deep dyspareunia. She has had two children by caesarean sections and a miscarriage with confirmed hydatidiform mole. There was no other relevant history. Examination revealed a large submucosal left paravaginal mass. Tumour markers [ CA 125, CEA, HCG, AFP] were all normal. A pelvic ultrasound scan revealed a complex cyst measuring 75 X 95 X 107 mm heterogenous in echotexture containing calcified and mainly solid areas within, and normal uterus and ovaries. No flow seen on power Doppler with a possible diagnosis of either dermoid or mucinous cystadenoma. MRI suggested an ovarian mass extending into left paravaginal space and periurethral area (fig. 1 & 2). It has characteristic features of a mucinous cystadenoma. The case was discussed at Gynaecological MDT meeting and decision made to operate in conjunction with urologists. Ureteric stenting was performed. At laparotomy a 11 cm mass extending to left lateral paravaginal space and deep in pelvis was found. A total abdominal hysterectomy and bilateral salpingo-oophorectomy with removal of left pelvic sidewall mass was undertaken. As the ureter was passing medially over the cyst, the pelvic sidewall had to be opened and the ureter dissected clear. In addition the bladder and vagina were dissected more extensively. The patient was transferred to HDU. Post-operatively she had persistent haematuria. A cystogram and retrograde ureterogram performed were normal. Ureteric stents were removed two days post-op and she was discharged on day 9. Her dyspareunia had resolved and cautionary MRI at 6 months was normal. Histologyof the specimen sent showed a cyst lined by normal stratified squamous epithelium. Sebaceous glands were also present. A large amount of keratin debris was noted (fig. 3). This has therefore confirmed the cyst to be a dermoid. Discussion: There are only a handful of reported cases of paravaginal dermoid cysts in the literature but none have the dimensions as described in our case. Also the presentation in this lady is somewhat unusual. There was a reported case of recurrent paravaginal cyst following a right mediolateral episiotomy which had to be excised. It had elements suggestive of a dermoid2. Siu et al3 described a case of a 29 year old woman who presented with a 6cm paravaginal wall cyst which was excised and histological examination confirmed it to be a dermoid. However they mentioned the challenges of ultrasound features in differentiating between a dermoid and epidermal inclusion cyst. Although it has been suggested that a distinct hyperechoic nodule is pathognomonic of a dermoid cyst4 however these can be mistaken for bowel contents or a hemorrhagic cyst. MRI can be a useful tool in these situations as dermoid cyst exhibit high signal intensity and these cyst can be differentiated from malignant masses5. Ultimately the diagnosis will rely upon histological examination of the specimen as with this case. This case also highlighted the surgical challenges of a benign cyst given the position it occupied within the pelvis. A multidisciplinary-team approach including pre-operative work-up, reviews of imaging, opinions of various specialties as well as involvement of the gynaecological oncologists and urologist were fundamental to the desired outcome in this patient as it is demonstrated by the extensive dissection involved in mobilising the cyst. Ureteric stenting intraoperatively proved invaluable in delineating appropriate structures due to the close proximity of this cyst to the pelvic sidewall and bladder. These cases should therefore be done in conjunction with gynaecological oncologists. Figure 1. MRI (T2-weighted sagital section) showing the cyst to be displacing left lateral border of bladder and urethra anteriorly and to the right. However there is a clear plane separating the two. There is no suppression of signal to suggest intralesional fat. Figure 2. Cyst is laying left of the vagina and the rectum is seen displaced to the right posteriorly (T2 axial) Figure 3. Dermoid cyst lined by stratified squamous epithelium filled with keratin debris. Sebaceous glands are also noted References: 1. Danforth’s Obstetrics and Gynaecology (10th ed). Gibbs RS, Danforth DN, Karlan BY, Haney AF. Lippincott Williams and Wilkins: Philidelphia, 2008; 1022 2. Hirose R, Imai A, Kondo H, Itoh K, Tamaya T. A dermoid cyst of the paravaginal space. Arch Gynecol Obstet 1991; 249:39–41. 3. Siu SS, Tam WH, To KF, Yuen PM. Is vaginal dermoid cyst a rare occurrence or a misnomer? A case report and review of the literature. Ultrasound Obstet Gynaecol 2003; 21(4): 404-406 4. Quinn SF, Erikson, Black WC. Cystic ovarian teratomas: the sonographic appearance of the dermoid plug. Radiology 1985, 155: 477-478 5. Bazot M, Daraï E, Nassar-Slaba J, Lafont C, Thomassin-Naggara I. Value of magnetic resonance imaging for the diagnosis of ovarian tumours: a review. J Computer Assisted Tomography.2008;32(5):712–723