Download
1 / 32
350 likes | 1.38k Views
Bronchiolitis Obliterans Organising Pneumonia (BOOP), G ranulomatosis with Polyangiitis. פרופ' נוויל ברקמן מכון הריאה ביה"ח האוניברסיטאי הדסה עין-כרם. Brochiolitis Obliterans and Organising Pneumonia (BOOP). Clinico- Pathological Diagnosis Clinical Radiological Pathological.

E N D
Bronchiolitis Obliterans Organising Pneumonia (BOOP), Granulomatosis with Polyangiitis פרופ' נוויל ברקמןמכון הריאהביה"ח האוניברסיטאי הדסה עין-כרם
Brochiolitis Obliterans and Organising Pneumonia (BOOP) • Clinico- Pathological Diagnosis • Clinical • Radiological • Pathological
Brochiolitis Obliterans and Organising Pneumonia (BOOP)Differential Diagnosis • Idiopathic (Cryptogenic Organising Pneumonia) • Infection • Post-transplantation • Collagen vascular disease • Irradiation • Drugs • Other
Idiopathic BOOP (Cryptogenic Organising Pneumonia) • M=F, any age (mean 58). • Acute or subacute onset of cough, fever, fatigue, weight loss, dyspnea "slowly or non-resolving pneumonia" • Inspiratory crackles, leukocytosis, raised ESR • X-ray: Bilateral diffuse alveolar infiltrates, peripheral, nodular, lower lobes, pleural effusion is rare.
COP- cont. • PFTs: restriction, reduced diffusion, obstruction (20%), hypoxemia. • Diagnosis: characteristic pathology with fibrotic buds in alveoli (organising pneumonia) and bronchiolitis obliterans. • Treatment: Steroids, cyclophosphamide. • 2/3 respond, others have progressive disease.
Pulmonary Vasculitis • Granulomatous vasculitis syndromes • Granulomatosis with polyangiitis (GPA) Wegener's vasculitis • Eosinophilic Granulomatosis with polyangiitis (EGPA) Churg-Strauss vasculitis • Lymphomatoid granulomatosis • Pulmonary-renal syndromes • Microscopic polyangiitis (overlap polyangiitis syndrome) • pauci-immune glomerulonephritis • Classical polyarteritis nodosa • Giant cell arteritis • Takayasu's disease • Behcet's disease
Granulomatosis with polyangiitis (GPA)Definition • A multi-organ disease histologically characterized by necrotizing vasculitis involving the small vessels, extensive necrosis & granulomatous inflammation
Granulomatosis with polyangiitisClinical manifestations Hoffman GS: Ann Intern Med 1992;116:488
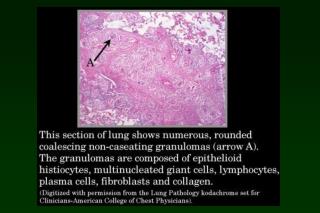
Granulomatosis with polyangiitisPathology • Necrotizing vasculitis: arterioles, venules & capillaries • Granulomatous inflammation • Geographical parenchymal necrosis • Hemorrhagic infarcts • Fibrosis
Granulomatosis with polyangiitisTreatment • Mortality >80% within 3 years without adequate treatment • Treatment of choice: • Prednisone 1mg/kg/day • Cyclophosphamide 1-2mg/kg/day (orally) • Remission is achieved in 70-93%
Eosinophilic granulomatosis with polyangiitisChurg-Strauss syndrome • History of asthma • Marked blood eosinophilia (up to 10000/ul) • Vasculitis, eosinophilic tissue infiltration • Sinusits • Skin (70%)- nodules,purpura, urticaria • Nervous system- mononeuritis muliplex (66%), CNS • GIT- abdominal pain (60%), diarrhea (33%), bleeding • Cardiac- cardiac failure (50%), pericarditis, hypertension • Renal- dysfunction (50%) • fever, lymphadenopathy
Churg-Strauss cont. • Lungs- infiltrates (>70%), usually transient and patchy, also nodules , interstitial infiltrates, pleural effusion (1/3). • Obstructive PFTs, elevated IgE, anemia, elevated ESR • BAL- eosinophilia (33%), eosinophils in pleural fluid • Biopsy- necrotising giant cell vasculitis (small arteries and veins), eosinophils, granulomas. • Treatment: Steroids, cyclophosphamide.
Rheumatoid ArthritisPulmonary manifestations • Pleural disease pleurisy (20%), effusion (4%), unilateral (80%), R>L middle-aged male, any time during the illness Associated with nodules not arthritis Fluid: exudate, LDH>1000, low glucose (<50mg% in 80%),low pH, lymphocytic, RF +, low complement
RA-cont. • Interstitial pneumonitis identical to idiopathic pulmonary fibrosis fullblown in 2%, abnormal PFTs in 41% M>F, patients are RF positive Cough, dyspnea, dry rales, clubbing hypoxemia, restrictive PFTs, reduced DCO Variable response to steroids Poor prognosis (survival 3-5 years) May be drug-induced (methotrexate, gold, penicillamine)
RA-cont. • Nodules: single (1/3) or multiple (2/3), more common in men related to disease activity and skin nodules asymptomatic, may cavitate, rarely hemoptysis peripheral, 0.3-7cm diameter may respond to steroids • Caplan's syndrome: pulmonary nodules with RA in coal miners (coal miner's pneumoconiosis)
RA-cont. • Bronchiolitis Obliterans airways obstruction, 60% of smokers, 30% of non-smokers peribronchial inflammatory infiltrate may be drug-induced • Pulmonary hypertension pulmonary arteritis
Systemic Lupus ErythematosisPulmonary manifestations • Pleura:- pleuritis or effusion, 50-75% of patients, presenting symptom in 1/3, fluid is an exudate, PMNs, raised ANF, LE cells • Interstitial pneumonitis:- acute (fever,cough, progressive hypoxemia) or chronic • Pulmonary thromboembolic disease:- lupus anticoagulant positive patients • Diaphragmatic dysfunction • Atalectasis:- subsegmental, bibasilar • INFECTION!
Goodpasture's syndrome • Alveolar hemorrhage • Glomerulonephritis • Anti-glomerular basement membrane antibody
Goodpasture's syndrome • Young males • Autoimmune disorder • Clinical features: Rapidly-progressive glomerulonephritis Hematuria, proteinuria, renal failure Hemoptysis, dyspnea, cough Anemia Arthralgia
Goodpasture's syndrome • Laboratory features: X-ray: transient infiltrates Urine:red cells, casts Iron-deficiency anemia Restrictive defect on lung-function tests with increased diffusion capacity. • Diagnosis: Hemosiderin-laden macrophages Anti-GBM antibodies Renal biopsy • Treatment: Plasmapharesis, steroids, cyclophosphamide.