Download
1 / 29
290 likes | 432 Views
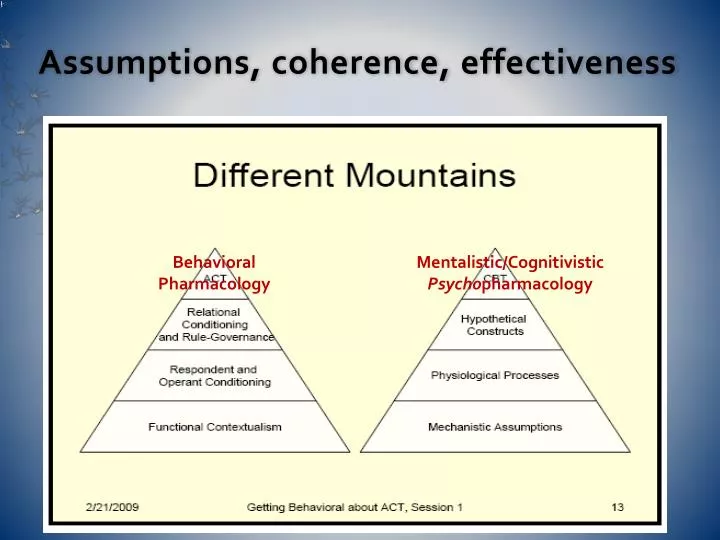
Assumptions, coherence, effectiveness. Behavioral Pharmacology. Mentalistic/Cognitivistic Psycho pharmacology. A Philosophical Structure for Psychiatry Kenneth S. Kendler AJP 2005.

E N D
Assumptions, coherence, effectiveness Behavioral Pharmacology Mentalistic/Cognitivistic Psychopharmacology
A Philosophical Structure for Psychiatry Kenneth S. Kendler AJP 2005 Seeks a coherent conceptual and philosophicalframework for psychiatry that consists of eight major propositions: • Grounded in mental experiences– thoughts, feelings, etc • Cartesiandualism is false (see however 3, 4, 6, 7) • Epiphenomenalism isfalse.thoughts, feelings, and impulses matter to science because they do things / have causal efficacy in the (real) world • Brain-mind & mind-brain causality real. Mental phenomenahave causal efficacy in the world. They affect our brains andbodies & through them the outside world.
RE – 2. Cartesian dualism is false We need toreject definitively the belief that mind and brain reflect twofundamentally different and ultimately incommensurable kindsof "stuff." in accord with overwhelming clinical and scientific evidence, we conclude that thehuman first-person world of subjective experience emerges fromand is entirely dependent upon brain functioning… The mentalworld does not exist independently of its physical instantiationin the brain. To accept monism means to no longer consider themental (or functional) to be a fundamentally different thingfrom the biological (or organic)… the mental and thebiological become different ways of viewing and/ordifferentlevels of analysis of the mind-brain system.
A Philosophical Structure for Psychiatry 2 5. Psychiatricdisorders are etiologically complex 6. Explanatory pluralism preferable to monisticexplanatoryapproaches, especially biological reductionism (?2) 7. Psychiatry needs to move from a prescientific "battle of paradigms"toward a more mature approach that embraces complexity alongwith empirically rigorous and pluralisticexplanatory models. “Ways of viewing a mind-brain system” 8. Need to accept "patchy reductionism" with thegoalof piecemeal integration in explaining complexetiologicalpathways to psychiatric illness a little bit ata time. … eliminating incoherence in assumptions?
What kinds of things are psychiatric disorders? Kendler, Zachar and Craver, Psychological Medicine, 22 Sep 2010Depts of Psychiatry, Psychology, and Philosophy-Neuroscience-Psychology Program Psychiatry etiology & underlying mechanisms: thus (MPC) kinds • Mechanistic Property Cluster(MPC) kinds; “a kind is real,the cluster of properties is lawfully connected independently of our classifications.” “…we take ourselves to be investigating an objective causal structure that is independent of our investigative and instrumental practices.” Complex, mutually reinforcing networks of causal mechanisms, objectively grounded features of causal structure of the mind/brain, fuzzy sets - mechanisms at multiple levels that act and interact Defining our disorders at the level of property clusters under-girded by dysfunctional but self-sustaining mechanisms is a practical goal. Indeed, we are seeing early signs of success of uncovering such mechanisms in contemporary research. (? C.f. actual evidence)
Philosophy of Psychopharmalogy. CUP 2008 Dan Stein. Previous work with David Kupfer, Schatzberg, Stephen Stahl Chapter 3 – How to think about science - Larger questions about science, language, medicine, and even about philosophy “What is a medical disorder?”, and perhaps the most important question in philosophy of psychiatry: “What is a psychiatric disorder?” 2 approaches (the classical approach) - well-delineated formal definitions of disorder (the critical approach) - arguments that no scientific response is possible (synthetic or integrative position) taken here draws on cognitive-affective science and emphasizes that the brain-mind is embodied sensorimotor-affective neuronal circuitry allows humans to interact with their physical and social world… (Conceptual Nervous System!) development of basic-level and abstract cognitive-affective maps (or metaphors) for understanding the world. (Mentalist CNS!!)
NIMH Research Domain Criteria (RDoC) project – AJPsychiatry Editorial July 2010 RDoC classification rests on three assumptions. • mental illnesses are brain disorders– i.e. disorders of brain circuits. • dysfunction inneural circuits can be identified with the tools of clinicalneuroscience, eg electrophysiology, functional neuroimaging,and new methods for quantifying connections in vivo. • data from genetics and clinicalneuroscience will yield biosignatures that will augment clinicalsymptoms and signs for clinical management. Example of circuitry-behavior relationships and futureclinical use:…"anxiety disorder" and data from imaging,genomic sequencing, & laboratory measures of fearconditioning and extinction to determine prognosis and appropriatetreatment, as in “Proper Medicine” now Key unspoken assumptions: healthy normality, ontological reality, correspondence based mechanist/biologist “truth”, objective science
CHEMICAL IMBALANCES – OR NOT After 40 years of research, in contradiction to prevailing beliefs, neurotransmitter theories have failed to achieve empirical support. “Although it is often stated with great confidence that depressed people have a serotonin or norepinephrine deficiency, the evidence actually contradicts these claims” Professor of Neuroscience E.Valenstein “…there is no “real” monoamine deficit” Psychiatrist Stephen M. Stahl “We have hunted for big simple neurochemical explanations for psychiatric disorders and have not found them” Kenneth Kendler “Thus… currently available agents likely restore mood by modulating distinct processes that are unrelated to the primary pathology of depression” Krishnan and Nestler, AJP in press 2010
NEUROCHEMICAL MECHANISMS? Linking Molecules to Mood - New Insight Into the Biology of Depression Krishnan and Nestler, American Journal of Psychiatry October 2010 • after more than a decade of PET studies (positioned aptly to quantitatively measure receptor and transporter numbers and occupancy), monoamine depletion studies (which transiently and experimentally reduce brain monoamine levels) , and genetic association analyses of polymorphisms in monoaminergic genes… • there is little evidence to implicate true deficits in serotonergic, noradrenergic, or dopaminergic neurotransmission in the pathophysiology of depression. (i.e. unrelated to the primary pathology) Molecular neuropharmacology. 2009 Nestler, Hyman and Malenka “Neurotransmitter-related hypotheses explaining the aetiology of schizophrenia are based purely upon pharmacological evidence, and thus are likely to be incomplete or misleading. … aberrations in these systems do not necessarily underlie psychotic disorders”
Psych0pharmacology – usual “truths” • - Thorazine arrived, and allowed the Asylums to empty in a psychopharmacological revolution, a step forward, and around the same time tricyclics discovered – ANTI psychotics/depressants Chemical imbalances – the presumption from drug neurochemical mechanisms to illness causes – excess dopamine, lack of serotonin 1987 – Prozac – the SSRI revolution, a major step forward 1988-91 – Risperidone, Clozapine – the atypical revolution 1999 – US Surgeon General Mental Health : A Report – “a wide variety of treatments of well-documented efficacy for the array of clearly defined mental and behavioral disorders … across the life span” … and further “advances in neurosciences and molecular biology”…
Psychopharmacology – historical facts Asylums emptied before drugs, those with drugs earlier - emptied later! No evidence for any role of dopamine excess or lack of serotonin etc 1955 – about 365,000mentally ill in US asylums – 1 in 470 people 1987 – SSI / SSDI recipients: 1.25 million – 1 in 184 people ($800 million) 2007 – SSI / SSDI recipients 4 million – a tripling ($30 billion, now $40 b) Every day in US 850 adults added to SSI / SSDI 1987 – 16,000 kids on SSI/SSDI – this is an apples to apples comparison 2007 – 600,000 kids on SSI/SSDI – 35 times as many THE PUZZLE – A REVOLUTIONARY ADVANCE AND AN EXPLOSION OF DISABILITY DUE TO MENTAL ILLNESS
New Zealand, Australia, Iceland NZ 2000 2010 rise of 23,142 48,899 18 - 64 year olds I.E. from 1 in every 168 to 1 in every 90on government disability (sickness or invalid benefits) in New Zealand due to psychiatric conditions % total disability due to psychiatric conditions 26% 34% total disability count rose 56,161 adults, 46% due to psychiatric conditions. • " bipolar spectrum disorder" US 4.4%, NZ 3.9%, India 0.1%, Bulgaria 0.3%. AUSTRALIA 2001 2010 rise of 140,965 227,420 adults I.E. rise of 1 in every 137 to 1 in every 98on disability due a psychiatric disorder % total disability due to psychiatric conditions 22.6% 28.7% of the total disability count increase, 51% due to psychiatric conditions. ICELAND 1992 2007 rise from 84 per 100,000 to 217 per 100,000 population in the new cases of disability annually due to mental and behavioral disorders
Recent effectiveness data STAR*D"largest antidepressant effectiveness trial ever conducted” NIMH trumpeted results – 67% remission, a great achievement The facts - 4041started SSRI, and after 4 trials, only 108 in remission and did not either have a relapse and/or dropped out by the end of 12 months of continuing care 2.7% 12 month remission The real results "point to a lack of long-term efficacy for antidepressants." Fake results said medications "far more effective" than placebo CATIE – maximum 20% continued meds over a year CUTLASS – older drugs better tolerated and better quality of life JAMA – haloperidol = olanzapine, with less cost, less fatal s/e’s Sz outcomes declined since 1970’s, now = 100 YEARS AGO.
STAR D – author responds to review "The overall cumulative remission rate was 67%“ Whereas the review found… “4041 patients started, 108 had a remission and did not either relapse and/or drop out by 12 months - i.e. only 2.7%” “I think their analysis is reasonable and not incompatible with what we had reported“
STAR-D more spin from authors Every drug, and combination of drugs showed same effect as every other drug, and drug combination. Despite making use of a wide gamut of medications, switching patients from a drug with one neurochemical action to another did not produce differential outcomes In contradiction to their data, the STAR*D authors claimed, “The findings are suggestive that major depressive disorder is biologically heterogeneous … different treatments differ in the likelihood of achieving remission in different patients”
STAR D – a small sample of the key authors’ financial disclosures…
SCHIZOPHRENIA OUTCOMES – Harrow et al, NEJM 2007, NIMH funded, no publicity…
Manic-depression outcome change…good poor in 40 years of drugs “in the era prior to pharmacotherapy, poor outcome in mania was relatively rare. . . …modern outcome studies found majority of bipolar patients with high rates of functional impairment.” “medication-induced changes” may be at least partly responsible. Antidepressants may cause a “worsening of the course of illness” and Antipsychotics “depressive episodes” and “lower functional recovery” Drug side effects, may “explain the cognitive deficits” HARVARD UNIVERSITY and ELI LILLY ARTICLE 2000
Manic-depression –good prognosis to poor over 40 years of the modern drug era “prognosis for bipolar disorder was once relatively favourable, but contemporary findings suggest that disability and poor outcomes are prevalent.” “neuropharmacological-neurotoxic factors” might be causing “cognitive deficits in bipolar disorder patients.” “As few as 1/3 of BPD patients achieve full social and occupational functional recovery to their own premorbid levels.” Further - Bipolar patients today suffer from a host of physical illnesses--cardiovascular problems, obesity, thyroid dysfunction, etc.--which, researchers admit, may be due to “toxicity from medications.”
Psychotropics and children Stimulants – no evidence of long term functional improvement “associated with worse hyperactivity-impulsivity and with oppositional defiant disorder symptoms,” and greater “overall functional impairment.” Anti-depressants - “recommending (any antidepressant) as a treatment option, let alone as first-line treatment, would be inappropriate.” Use of stimulants and antidepressants ? juvenile “bipolar illness” Until the 1990s, bipolar illness was rarely diagnosed in teenagers and virtually never in prepubertal children. Then… Stimulants and antidepressants to children psychotic and manic reactions and were then diagnosed with bipolar disorder. Child bipolar patients treated with antipsychotic meds “were significantly less likely to recover than those who did not receive a neuroleptic.”
CLINICAL GUIDELINE MANIPULATION American Psychiatric Association clinical practice guidelines for schizophrenia, bipolar disorder, and major depressive disorder 90% of authors had a financial tie to companies whose products were specifically considered or included in the guideline they authored. All of the companies whose drugs were listed as “optimal medications” for major depressive disorder provided funding to the authors of the guidelines for major depressive disorder.
Like old men often do...1boringoldman I am a psychoanalyst, a group that was disenfranchised with the rise of the psychopharmacological focus of modern psychiatry, but that didn’t hurt me personally, and it has been true for thirty years without getting me stirred up. The thing that brought me out of the woodwork is that I’m mad as hell about being being lied to. And I have been lied to, as have our patients. There’s nothing wrong with having drugs to use that are symptomatic rather than curative, weaker than we’d prefer, or more toxic than we’d choose. That’s true of medicine no matter what the specialty. It’s why medical training goes on so long [like a lifetime] – learning to get the most out of what’s available without hurting people. It’s the state of the art as they say. But as a doctor seeing patients, to do that, I have to have access to accurate information about medications.
I have been lied to, as have our patients I needed to know about medications after years of a psychotherapy practice away from the medication world. I went to "bone up." What I found was just not credible. In fact, a lot of it was just plain lies. The antidepressants sometimes cause akisthisia and suicidal ideation; regularly produce dreadful withdrawal symptoms; aren’t useful in kids; and are nowhere near as effective as advertised. I’m not mad about that. The drugs are what they are. I’m mad that I had to find out those things by myself. My colleagues in high places and the companies making the drugs knew about all of that, and they didn’t tell me. In many cases, they tried to keep me and my patients from knowing. .
Lying in a situation where the truth is vital I’m not mad that the Atypical Antipsychotics aren’t as good as we’d hoped. They’re no more efficacious than our older drugs; cause obesity and sometimes diabetes; have neurotoxicity not too different from the older neuroleptics; and produce withdrawal syndromes just like the antidepressants. I had to find out about those things all by myself. Same complaint – betrayed by formerly trusted resources, on purpose. That’s not a complaint about neuropsychopharmacologists or neuroscientists. It’s not a complaint about the pharmaceutical industry or even capitalism. It’s a complaint about people betraying the the only standard that separates medicine from the fantastic.It’s a complaint about lying in a situation where the truth is vital.
Crises aren’t just a time for growth or a change in direction They’re a time for correcting what’s been wrong As the egregious scandals have swept through psychiatry and psychopharmacology, our organizations have been way too passive, way too defensive, way too uninvolved and slow to embrace much needed reform. The known sinners in high places are still there. There’s a big difference between protecting one’s own kind and colluding with misbehavior that needs to be addressed decisively. Universities, Medical Schools, Professional Organizations, Scientific Colleges, even Governmental Agencies have ignored loud symptoms of ongoing disease during a time of epidemic. It looks from the outside like they’ve been bought out. I hope that’s not true, but whatever the case, the ball’s in their court now. No matter the cause for their failures in enforcement of ethical standards, this growing crisis is a time for new directions there too. We don’t need much reflection to know what needs changing in that department. We can’t move forward without acknowledging and addressing the failures of the recent past. There’s just no room for liars and entrepreneurs in a healthy psychiatry.
URGENT NEED FOR AN ALTERNATIVE “the drug effect on behavior was related to the schedule … the schedule is,as it were, the score of the symphony… These changes are sufficient to change themusic profoundly, making slow themes intofast and soft interludes into loud, even thoughthe drugs do not affect the symphony or thequality of the instruments. (Peter Dews, 1964)
BEHAVIORAL PHARMACOLOGY Behavioral pharmacology uses methods and concepts from behavior analysis to explore and explain the behavioral effects of drugs. Behavior analysis is a unique natural science approach to the study of behavior developed by B. F. Skinner, but since then refined and clarified philosophically (Steven Hayes, Aaron Brownstein, Linda Hayes, Dermot Barnes-Holmes, Kelly Wilson, etc) Because behavior analysis forms the theoretical and methodological foundation of behavioral pharmacology, it deserves careful attention. Because contextual behavioral science is our foundation, likewise attention The following review may clarify possibilities, and some of the reasons for the assumptions of functional contextualism, the position taken, why our flag is planted just here. In contrast to the dead ends of reductive mechanistic biologism.