Download
1 / 30
300 likes | 505 Views
Hemi Central Retinal Vein Occlusion. Grand Rounds March 11, 2005 John Nicolau, M.D. Leo Dominguez, M.D. CRVO/BRVO Findings. Most common retinal vascular problem second to Diabetic Retinopathy Dilated and tortuous veins in all 4 quadrants ONH Edema

E N D
Hemi Central Retinal Vein Occlusion Grand Rounds March 11, 2005 John Nicolau, M.D. Leo Dominguez, M.D.
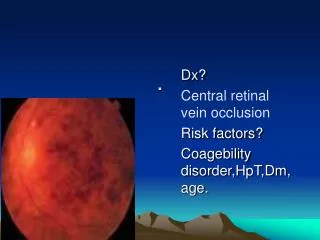
CRVO/BRVO Findings • Most common retinal vascular problem second to Diabetic Retinopathy • Dilated and tortuous veins in all 4 quadrants • ONH Edema • Diffuse retinal hemorrhages at all levels and possibly cotton-wool spots • Largely divided into ischemic vs. nonischemic by Fluorescein Angiography • BRVO Similar but segmental distribution of findings – morbidity related to area of blockage
Clinical Presentation • Abrupt decrease in vision/Resolution? • TVOs • Redness and Photophobia • Pain – usually advanced with NVI, NVG and increased IOP • Classic clinical picture on dilated examination
Pathophysiology • CRVO • Thrombosis at level of lamina cribosa possibly 2’/2 vessel narrowing and turbulent flow – relation to increased IOP? • Occlusion of arterial and venous components producing differing clinical pictures • BRVO • Compression of vein by artery sharing common adventitial sheath causing turbulence and thrombosis • Location of occlusion affecting clinical appearance
Risk Factors • CRVO • Systemic Hypertension • Cardiovascular Disease • Diabetes Mellitus • POAG • BRVO • Systemic Hypertension • Cardiovascular Disease • Glaucoma • Increased Body Mass Index at 20 yrs old • NOT Diabetes Mellitus • Hypercoaguable States
Causes of Vision Loss • CRVO/BRVO • Macular Edema • Macular Hemorrhage with RPE damage • Macular Nonperfusion • Neovascular Glaucoma (CRVO) • Retinal Neovascularization and complications (BRVO) • ERM • Macular Hole • RD • Subretinal Fibrosis
Prognosis and Statistics • CRVO • Approximately 30% ischemic (10 DD on FA) • NVG 40% to 60% of these eyes vs 5% Nonischemic • <10% developed retinal neovascularization • CVOS – 83% of undetermined developed ischemia or NVI • BRVO • 1/3 to 1/2 recover VA of 20/40 or better w/o therapy • 50% Ischemic (5 DD) of which 40% develop neovascularization; 60% of these develop VH • NVI Rare; 1%
Treatment of CRVO • Early studies with poor definition of ischemia, non randomization, lack of controls, small number of subjects, etc. • CVOS founded and attempted to answer two main questions: • 1. Whether PRP prevents NVI and NVG in ischemic eyes • 2. Whether grid treatment improves VA in eyes losing vision from macular edema
Perfused and Indeterminate Groups • 34% of initially perfused eyes converted to nonperfused and thus became eligible for the study • Final VA depended on initial VA • 16% developed iris/angle neovascularization • Strongest risk factors were degree of nonperfusion and VA < 20/200 • 20/52 of indeterminate group developed neovascularization
Macular Edema • Eyes with initially 20/50 VA or worse showed no difference in final VA after grid-pattern treatment compared to control eyes which received no treatment. Macular edema was however reduced in these eyes angiographically.
Nonperfused Group • Set out to determine if prophylactic PRP would prevent neovascularization or it was more appropriate to wait for its development • Neovascularization developed less in treated eyes but not with statistical significance • Regression was prompt when treated in both controls and treated eyes
Recommendations • There is no indication for PRP in ischemic or nonischemic eyes without neovascularization if patient available for follow up • Grid treatment not shown to improve VA in eyes with decreased VA due to macular edema • Progression towards ischemia greater in early months following CRVO with VA <20/200 best indicator • Monthly follow up for first 6 months with prompt PRP when any neovascularization observed • No systemic anticoaugulation
BRVO Treatment • BVOS • Found that 63% of treated eyes with perfused macular edema, no foveal heme, and other minor criteria gained two or more lines of VA when compared to controls at 3 years. • PRP reduced VH in half (60% to 30%) when neovascularization present
BRVO Recommendations • Wait 3 to 6 months before beginning laser therapy in an eye with VA < 20/40 and perfused macular edema • No treatment for macular nonperfusion • PRP at first sign of NVD, NVE, or NVI
HCRVO • CRVO with two trunks behind lamina cribosa (20%) • Thought to be variant of CRVO but with complications and findings of both types of vein occlusions • Also divided into ischemic and nonischemic
HCRVO/CRVO Similarities • Hayreh and Hayreh found BRVO artery crosses over vein in 91% whereas in HCRVO only 1/3 showed this and >1/3 had no crossing • Collateral vessels in BRVO feed at crossing whereas in CRVO they form at disc or more posterior as found in HCRVO • In HCRVO about 1/3 showed increased IOP as did CRVO unlike BRVO where increased IOP not > general population • ONH edema seen in HCRVO/CRVO but not usually in BRVO • Lack of NVI/NVG in BRVO not found it HCRVO/CRVO
Further Evidence • Appiah, Clement Trempe found increased IOP when comparing HCRVO and CRVO but not BRVO and the above • Also found HTN and Hyperopia in BRVO but not CRVO or HCRVO • Hayreh, Zimmerman et al. compared HCRVO and CRVO and found increased prevalence of glaucoma and OHT when compared to general population
Treatment Implications • HCRVO (ischemic) 13% NVI (Hayreh) thus NVI being > BRVO and < CRVO; • Nonischemic showed no neovascularization • NVD 29% and NVE 42% in ischemic HCRVO > CRVO and BRVO • Question arises as whether to pre-treat ischemic HCRVO with PRP and whether or not to treat macular edema in light of recommendations in BRVO but not CRVO
References • 1. BCSC. Retina and Vitreous. Section 12 pp 136-145., 2004. • 2. Spalton, David. Atlas of Clinical Ophthalmology; Retinal Vascular Disease I. pp 233 -243. 2004. • 3. Weinberg, David V., Venous Occlusive Diseases of the Retina. Principles and Practice of Ophthalmology. pp. 1887-1987. • 4. Clarkson, John G. Central Retinal Vein Occlusion. Retina. Vol 2. pp. 1368-1374. 2001. • 5. Finkelstein, Daniel and Fekrat, Sharon. Branch Retinal Vein Occlusion. Retina. Vol 2. pp. 1376-1381. 2001. • 6.Hayreh, S.S., Zimmerman, M. Bridget, Beri, Meena. Intraocular Pressure Abnormalities Associated with Central Retinal Vein Occlusion. Ophthalmology. Vol 111. Number 1. Jan 2004. 133-139 • 7. Appiah, Aaron, Trempe, Clement. Differences in Contributory Factors among HCRVO, CRVO, and BRVO. Ophthalmology. Vol 96 Number 3 March 1989. pp 364-366. • 8. Hayreh, S.S. and Hayreh M.S. HCRVO: Pathogenesis, Clinical Features, and Natural History. Archives of Ophthalmology. Vol 98. Sept 1980. pp 1600-1608. • 9. Alexander, J. Larry. Primary Care of the Posterior Segment. Retinal Vascular Disease. Pp 219-221. 1994.