Download
1 / 13
160 likes | 288 Views
“Is Immediate Chest Radiograph Necessary After Central Venous Catheter Placement in a Surgical Intensive Care Unit?” Dept of Surgery, University of Utah Medical Center. Shawn S. Carter January 2007 MIV Radiology. Why This Study was Conducted. Standard practice and FDA dictations:

E N D
“Is Immediate Chest Radiograph Necessary After Central Venous Catheter Placement in a Surgical Intensive Care Unit?”Dept of Surgery, University of Utah Medical Center Shawn S. Carter January 2007 MIV Radiology
Why This Study was Conducted • Standard practice and FDA dictations: • Obtain chest radiograph after CVC placement • At their institution, $98 charge per CXR • Estimated $300 million in charges annually from ONLY the post-procedural CXR
Methods • Prospective data recorded for 184 CVC placements in 1998 and 1999 • Also, chart review from 174 CVC placements during same time period but data sheets were not filled out • Thus, sample size N = 358
Types of CVC Placement Complications • Catheter Malposition • Hemothorax • Pneumothorax • Cardiac Tamponade • Vascular Erosion • Chylothorax • Arrythmia • Death
Results • Overall incidence of a complication: 9% • Catheter malposition most frequent complication • Two pneumothoraces occurred • Neither one diagnosed on post-procedural CXR
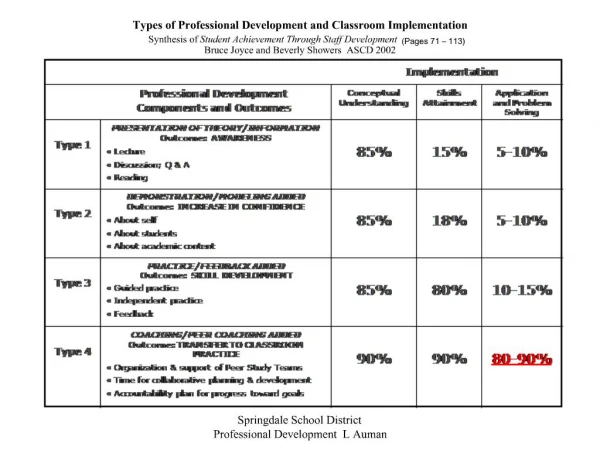
Within Prospective Group Refers to Incidence of a Complication
Conclusion Number One • “Straightforward” CVC placements with fewer than 3 needle passes yielded a complication likelihood of approximately 5%, with nearly all complications related to catheter positioning suggesting that an experienced surgeon can safely perform CVC placements.
Conclusion Number Two • The post-procedural chest radiographs did NOT diagnose the rare, but life-threatening Pneumothoraces that were later noticed on the scheduled daily CXR. Hence, the post-procedural benefit wasnil.
Audience Commentary • No mention of attorney’s angle as to the standard of practice • To which faculty members would this new policy apply • Feasibility of coordinating the timing of the CVC placement to the daily CXR
Special Thanks For Who Made This All Possible… • Dr. Neuffer • Department of Radiology • Class of 2007 • And all the Little People (FRED LIPATA)