Download
1 / 12
120 likes | 266 Views
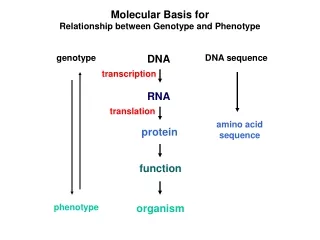
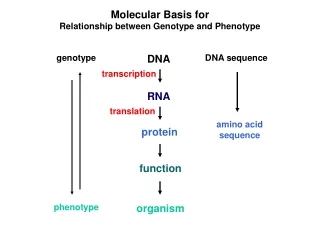
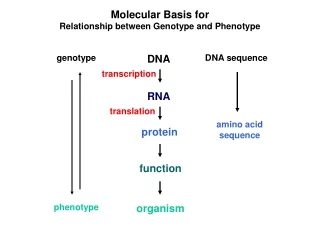
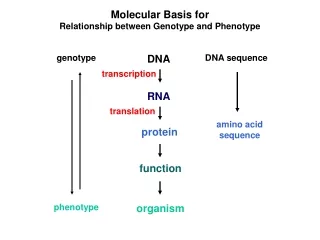
Discuss the relationship between phenotype and genotype in Fragile X syndrome. Louise Williams 06/03/2008. What is Fragile X syndrome?. Most common form of inherited cognitive impairment Autosomal dominant inheritance Classical Fragile X Syndrome

E N D
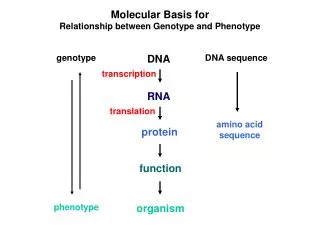
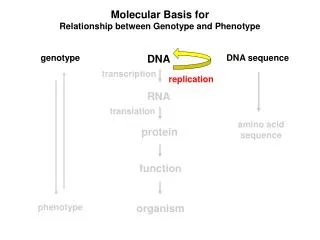
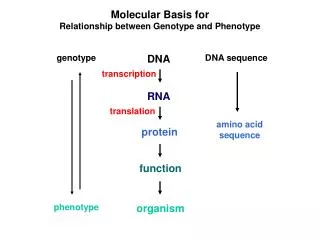
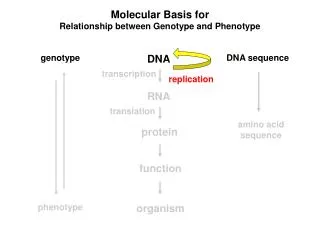
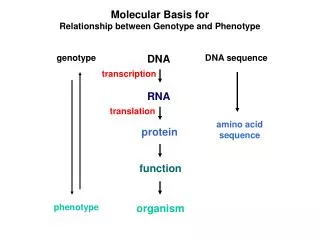
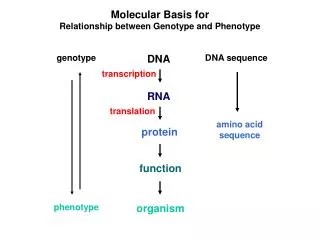
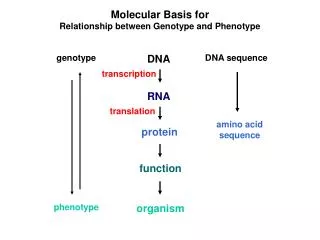
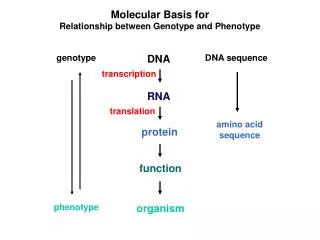
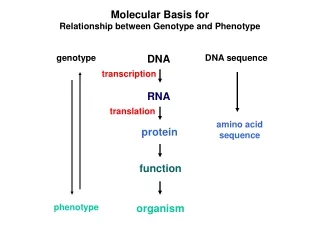
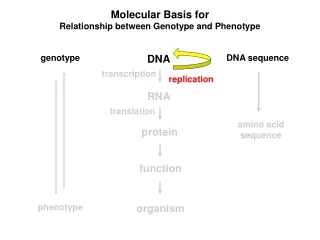
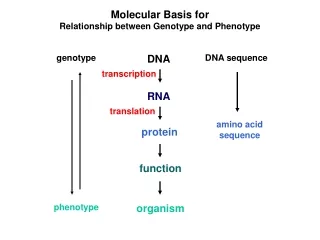
Discuss the relationship between phenotype and genotype in Fragile X syndrome. Louise Williams 06/03/2008
What is Fragile X syndrome? • Most common form of inherited cognitive impairment • Autosomal dominant inheritance • Classical Fragile X Syndrome • Mild to severe mental retardation (IQ 20-60), prominent jaw, large ears, macroorchidism, autistic spectrum behaviour, hand flapping, soft smooth skin • Other disorders associated with the FMR1 CGG repeat - FXTAS and POF
Genetics of Fragile X • 99% - Expansion/Methylation of CGG repeat in exon 1 of FMR1 which causes lack of protein product • Some cases caused by deletions or missense mutations confirming lack of protein is cause of disease • Alleles of FMR1 are categorised according to CGG repeat number • Normal alleles = 5-40 • Intermediate alleles = 41-58 (grey zone) • Premutation alleles = 59-200 • Full mutation = >200
‘Normal’ alleles • Normal alleles are stably transmitted without any increase or decrease in size/repeat number • In these alleles, the CGG repeat is interupted every 9-10 repeats by an AGG which maintains integrity • These alleles tend to be transmitted stably • Any change in repeat number tends to be small • The number of pure (CGG) repeats in a tract determines its stability – pure repeats of more than 35 uninterrupted CGGs are more likely to become unstable Intermediate alleles
Premutation alleles • Alleles of this size may be associated with subtle symptoms, but increase risk of FXTAS and POF • Expansion of premutation alleles to full mutation alleles only occurs on maternal transmission • Women with alleles in this size range are said to be at risk of having an affected child due to the potential for the allele to expand
Full mutations • Males generally have moderate to severe learning difficulties with or without other features • 50% of females will be affected, although more mildly than males • This is due to the ratio of active to inactive FMR1 in the brain which results from X inactivation
Mosaicism • 15-20% of FMR1 mutations are mosaic • 2 types of moaicism • Repeat size mosaicism • Both full and pre mutations are present • Methylation mosaicism • Full mutations variably methylated • These individuals will be affected but tend to be higher functioning • There have also been reports of unmethylated full mutation males who also tend to be higher functioning
Anticipation • Like other triplet repeat disorders, Fragile X shows anticipation • This occurs when less severely affected premutation carriers or full mutation mosaics transmit unstable alleles • This is not ‘classical’ anticipation as seen in other disorders, as premutation alleles can be transmitted stably for generations
Fragile X-associated tremor/ataxia syndrome • Late onset progressive cerebellar ataxia and intention tramor • Affects both males and females • Associated with premutation alleles • Shows age related penetrance in males (overall 40% at >50 yoa) • Lower risk in females
Premature ovarian failure • Cessation of menses at <40 yoa • Associated with high normal and intermediate alleles • 21% compared to 1% in general pop • Risk increases with repeat size but plateaus after about 100 • 59-79, 6.9; 80-99, 25.1; >100, 16.4
Conclusion • Size or classification of FMR1 CGG repeat generally correlates with fragile X syndrome phenotype (other than mosaicism) – Not surprising really, as alleles have been allocated according to their phenotype • Additional phenotypes found more recently to be associated with the expansion do not fall neatly into these brackets
References • Reference given in question • Gene Clinics