Download

1 / 0
50 likes | 479 Views
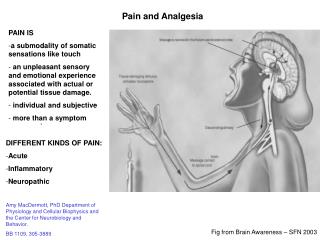
PRINCIPLES OF PAIN MANAGEMENT & ANALGESIA. “ thERE IS NO COMING TO CONSCIOUSNESS WITHOUT PAIN.” -CARL JUNG. PRINCIPLES OF PAIN & ANALGESIA. WHAT IS PAIN? An unpleasant sensory or emotional experience associated with actual or potential tissue damage

E N D