Download
1 / 33
370 likes | 663 Views
Genomics of Adverse Drug Reactions: The Need for a Multi-Functional Approach. Munir Pirmohamed David Weatherall Chair of Medicine and NHS Chair of Pharmacogenetics Department of Molecular and Clinical Pharmacology University of Liverpool. Adverse Drug Reactions: Classification.

E N D
Genomics of Adverse Drug Reactions: The Need for a Multi-Functional Approach Munir Pirmohamed David Weatherall Chair of Medicine and NHS Chair of Pharmacogenetics Department of Molecular and Clinical Pharmacology University of Liverpool
Adverse Drug Reactions: Classification • ON TARGET REACTIONS • Predictable from the known primary or secondary pharmacology of the drug • Clear dose-dependence relationship within the individual • OFF TARGET REACTIONS • Not predictable from a knowledge of the basic pharmacology of the drug and can exhibit marked inter-individual susceptibility • Complex dose-dependence
Outline • Phenotyping • Sample sizes • Genomic approaches • The path to clinical translation • Genetic exceptionalism
Genetic Contribution • Many factors predispose to adverse drug reactions, many of which are environmental and clinical • We do not know the overall genetic contribution to the occurrence of adverse reactions • The genetic effect will vary according to drug and reaction • ADRs account for: • 6.5% of all hospital admissions • 15% rate in in-patients • 8000 NHS Beds in the UK
Deep Phenotyping • ADRs can affect any organ system, can be of any severity – MIMIC OF DISEASE • Important to be aware of the phenotypic heterogeneity – link between clinicians and genomics experts • Although overall burden of ADRs is high, the incidence of individual ADRs may be low or rare in many instances – so patient identification can be difficult (cf. Type 2 Diabetes)
Power of Studies • Many pharmacogenetics studies in the past had small sample sizes, compunded by poor phenotype • Led to low effect sizes with lack of replication in independent cohorts • But since ADRs may be uncommon, it will never be possible to attain samples sizes seen in complex diseases • International consortia • Electronic medical records Toxic epidermal necrolysis 1 in million per year
InTernational Consortium on Drug Hypersensitivity (ITCH) • 12 international centres • 50 UK centres • 1500 patients Sponsored by the International Serious Adverse Event Consortium (iSAEC)
Electronic Medical Records: Clinical Practice Research Datalink • Previously GPRD • 12 million patient records (March 2011) Increased to 52 million with the transition to CPRD • Feasibility study using statin myopathy as paradigm • 641,703 patients prescribed a statin • 127,209 with concurrent CPK measurement
The R&D Governance Burden Statin myopathy Identified via CPRD Link to DNA samples 132 R&D approvals
Implicated SNP is in the SLCO1B1 gene (transporter) Shown with simvastatin 40mg and 80mg
Statin Myopathy GWAS All myopathy (n=128) vs. WTCCC2 (unimputed) SLCO1B1
Carbamazepine Hypersensitivity • More complicated than abacavir hypersensitivity • Different phenotypes • Skin (mild → blistering) • Liver • Systemic (DRESS) • Predisposition varies with ethnicity and phenotype • HLA-B*1502 (Chinese) • HLA-A*3101 (Caucasian)
CPT, 2012 HLA-B*1502
Replicated in Japanese, Chinese, South Korean, Canadian and EU populations • NNT = 47 • SmPC/drug label changed (for information) • Patient and clinician preferences • Cost effectiveness • 55% likelihood • Cluster RCT being planned Liverpool 22 patients with HSS
Whole Genome Sequencing in CBZ Hypersensitivity N= 48 (28 CBZ-induced severe hypersensitivity and 20 tolerant controls)
HLA-A* Loci Using NGS data • 30 HLA-A* loci typed • 18 HLA-A* alleles identified • 40% CBZ hypersensitive patients are A*31:01 positive
T Cells in Carbamazepine Hypersensitivity: HLA-A*31:01+ patient Clinical data Lymphocyte transformation test
Carbamazepine-Responsive T-cell clones FasL IFNγ IL-13 Perforin Granz.B 0 Specificity and Phenotype CBZ FasL IFNγ IL-13 Perforin Granz.B Secretion of cytokines and cytolytic molecules a) CD4+ TCC 0 CBZ b) CD8+ TCC
HLA Restriction of CBZ-Specific TCC MHC restriction of CD4+ (a) and CD8+ (b) TCC b) CD8+ (n=3) a) CD4+ (n=3) * p = 0.03 * p = 0.03 ns HLA class II restriction of CD4+ TCC HLA A31 restriction of CD8+ TCC ns * p = 0.03 n = 3 n = 3 p = 0.008 ** p = 0.004
Hierarchy of Evidence What type of evidence is required for demonstration of clinical utility?
Association with HLA-B*5701 Clinical phenotype Clinical genotype Technology-Based Reduction in the Burden of ADRs: The Case of Abacavir Hypersensitivity
Drug label changed before prospective study Two prospective studies did not contradict previous data from retrospective studies
Evidence standards differ between non-genetic and genetic tests • 3 examples given: • Drug exposure • Prevention of adverse drug reactions • Health technology assessment
Drug Exposure: Differential Evidential Standards • Example: Aztreonam SmPC • “after an initial usual dose, the dosage of aztreonam should be halved in patients with estimated creatinine clearances between 10 and 30 mL/min/1.73 m2” • Many different examples in hepatic and renal impairment with dose instructions based on PK studies and occasionally PK-PD modelling • No need for RCTs – in fact, would be impractical • However, a genetic polymorphism leading to same degree of change in drug exposure is often ignored and/or RCT data are required for implementation
Differential Evidence Standards • Unfamiliarity with genetic tests • Lack of experience in interpretation • Perceived cost of genetic testing • Lack of availability of tests • Poor turnaround time recommendations on dosing evaluation in patients with polymorphisms in known metabolic pathways
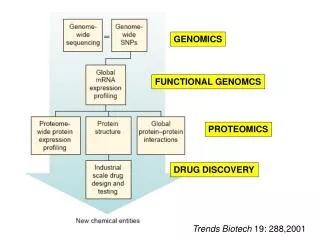
Summary • Prediction of adverse drug reactions (safety biomarker) • Insights into mechanisms of the adverse drug reaction Poste, Nature, 2011
“Hierarchies of evidence should be replaced by accepting—indeed embracing—a diversity of approaches..... ...It is a plea to investigators to continue to develop and improve their methods; to decision makers to avoid adopting entrenched positions about the nature of evidence; and for both to accept that the interpretation of evidence requires judgment.”
Acknowledgements • The University of Liverpool • B Kevin Park • Ana Alfirevic • Maike Lichtenfels • Dean Naisbitt • Ben Francis • Dan Carr • Ann Daly (Newcastle University) • Panagiotis Deloukas (Sanger Institute) • SERIOUS ADVERSE EVENT CONSORTIUM • EPIGEN • EU-PACT • FDA • Funders: Dept of Health (NHS Chair of Pharmacogenetics) • MRC, WT, DH, NIHR, EU-FP7