Download
1 / 60
610 likes | 734 Views
Using functional genomics to understand pain. Professor Rodney J. Scott Director of Genetics, Hunter Area Pathology Service. Max MB and Stewart WE (2008) The Molecular epidemiology of pain:A new discipline for drug discovery. Nature Reviews 7:637-658

E N D
Using functional genomics to understand pain Professor Rodney J. Scott Director of Genetics, Hunter Area Pathology Service
Max MB and Stewart WE (2008) The Molecular epidemiology of pain:A new discipline for drug discovery. Nature Reviews 7:637-658 • Watkins LR and Maier SE (2003) Glia: a novel drug discovery target for clinical pain. Nature Reviews 2:975-985
Definition of a Genetic Influence • Inherited predispositions to disease • Dominant disease effect (with modification) • Inherited traits that only become apparent when the • appropriate environment is present. Disease does not • develop UNLESS environmental exposure occurs • Gene-Gene interactions important in dictating disease • response and outcomes
Environment • Host • metabolism (e.g. estrogen metabolism) • normal functioning (e.g. neurotransmitters) • aging • External • infection • carcinogen exposure • life style
Phenotype Genotype Environment
Most diseases are multifactorial: Genetic predispositions, environmental factors, result in genetic changes that play a role in disease development throughout life Stroke Cancer Cardiac diseases Blood pressure Asthma Diabetes Infectious diseases Neuropathies Obesity Psychiatric conditions Hyperlipidaemia Pain
Molecular Epidemiology of Pain • Cost estimated to be ~ $ 1 Trillion annually in US • Common pain treatments have changed little over 30 years • Should be a tractable area for drug development – unique chemical mediators • Traditional research has focused on ~ 200 molecules (<1% of the genome) • Several novel drug classes that relieve pain in animal models have failed in clinical evaluation • Despite intensive efforts, clinical pain control has remained a puzzlingly elusive target. • Genomic studies in humans might compensate for the limitations of animal studies
Cell Types & Pain • Neurons have been the centre of attention • Glia Cells (micro glia cells and astrocytes) originally considered to support neuronal activity, should also be considered as they release a wide variety of molecules on stimulation • Glia dynamically modulate the function of neurons under both physiological and pathological conditions • Garrison et al. reported that peripheral nerve damage that created exaggerated nociceptive responses (neuropathic ‘pain’ behaviours) also activated spinal cord glia
Garrison et al demonstrated that astrocytes in spinal cord were activated (as reflected by immunohistochemistry for the astrocyte-specific activation marker, glial fibrillary acidic protein) in response to sciatic nerve damage.
Glia • Glia cells are stimulated by cytokines and chemokines • IL1, TNF & IL6 are pro-inflammatory cytokines that activate glia • IL10 is an anti-inflammatory cytokine that blocks the action of IL1 and IL6 • All 4 cytokines harbour functional polymorphisms that alter their activity
Genomic Studies • There is heterogeneity in the sensation of pain – suggestive of variance in the molecular mechanisms underlying the sensation • Variance in pain sensation is likely to be a result of genetic differences between individuals • Genomic studies on pain might reveal more than that identified in animal models • Under- or over-expression of target proteins in different pain phenotypes can be evaluated before clinical trials. • Genome wide studies of other disease have revealed novel genes in a wide variety of disorders • Macular degeneration, Crohn’s Disease, Cancer, Diabetes, etc…
Genomic Studies into Pain • Heritability of pain • Animal studies clearly indicate difference in pain thresholds – different mouse strains indicate 30% – 76% (median 46%) heritability • Human studies (Twin studies) • Monozygotic twins should be similar w.r.t. pain thresholds; Dizygotic twins will demonstrate normal sibling variance (even though they have a shared environment). • Variability in pain processing
Genomic Studies into Pain • Case-Control Studies of familial aggregation • Suitable for common pain conditions (back pain or migraine) – large number of cases • Identify cases from clinical records • Control subjects from the general population • Compare heritability • Frequency of pain in one population (this includes family members) compared to the other
Genomic Studies into Pain • Candidate Gene Studies • Many potential modifiers of pain sensation • Many cell types involved • Functional polymorphisms exist in genes involved in pain sensation • Promoter gene polymorphism inappropriate protein expression or loss of control fidelity • Polymorphisms in exons change of function • Alter miRNA controlling species
Association of COMT haplotypes with experimental pain sensitivity and with rate of metabolism of catecholamines (HPS = high pain sensitivity, APS = average pain sensitivity and LPS = low pain sensitivity)
Gene Expression in Rats after nerve injury Pain protective effects of the GCH1 haplotype in patients after discectomy Association of GCH1 haplotypes with human chronic spinal nerve root pain, experimental pain and synthesis of biopterin (essential for NO production
Genomic Studies into Pain(the identification of new biomarkers)
Biomarker Discovery • Define the question you wish to ask • There are many biomarkers both known and unknown • Determine the number of samples you need to answer the question (power calculation) • Ensure that there are sufficient sample sets for replication studies
Definition of a Biomarker • Quantitative Trait • Assess the risk of disease • Better define the disease • Define response to treatment • Assess the risk of recurrence
Definition of a Biomarker ctd. • Quantitative trait: • inheritance of a phenotypic characteristic that varies in degree and can be attributed to the interactions between two or more genes and their environment e.g. height, blood pressure, pain
Definitions: Environment: The sum total of all conditions and elements which make up the surroundings and influence the development and actions of an individual. Gene: a segment of a DNA molecule that contains all the information required for synthesis of a product (protein or RNA molecule), the deficiency of which may only become apparent after exposure to an appropriate environment.
The Human Genome ATCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGATGCCTAGGTGGCGAAATTGCAGAGTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGAACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTCGGACCTTAGAGCCTAGGTGGTCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGATGTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAACCCATTGCAGAGTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTTCGGACCTTAGAGCAGAGCCTAGGTGGCGAAATTGCAGAGTTTTAGAGCCTAGGTGGCGGCCTAGGTGGCGAAATTGCAGAGTTTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGCCTTAGAGCCTAGGTGGCGAAATTATCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGATGCCTAGGTGGCGAAATTGCAGAGTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGAACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTCGGACCTTAGAGCCTAGGTGGTCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGATGTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGA ACCCATTGCAGAGTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTTCGGACCTTAGAGCCTAGGTGGCGAAATTGCAGAGTTGACCTTAGAGCCTAGGTG ca. 3 billion base pairs ca. 25,000 Genes
Genetic Variability 99,9% identical 0,1% different > 10 Million Sequence variants
Different Types of DNA Sequence Variation • Differences in the copy number of repeated sequences (Tandemly repeated DNA): Satellite DNA (large arrays) Minisatellite markers (VNTR) Microsatellite Markers: di-, tri-, tetra- nucleotide markers • Interspersed repetitive DNA (retrotransposons): LINEs Long Interspersed Nuclear Elements (Alu) SINEs Short Interspersed Nuclear Elements (L1) transposable elements • Small Insertions and Deletions (Copy Number Variations or CNVs) • Single nucleotide polymorphisms (SNPs) markers: 90% human genome variations are single nucleotide changes
Mutation Rare sequence variants Presence in the population: <1% Great influence on disease development Sequence variations Polymorphisms • Common sequence variants Present in the population: >1% • Weak of no influence on disease development ACTTACGATTA ACTTACGCTTA Single Nucleotide Polymorphism (SNP)
Consequences of Mutation • Genetic Variability: adaptation, evolution • Deleterious mutation: Inborn error -- embryonic lethal. Germ cells -- hereditary disease Somatic cells -- malfunctioning of genes malignancies, atherosclerosis, etc.
...C C A T T G A C... …G G T A A C T G... ...C C G T T G A C... …G G C A A C T G... What is a SNP? Example order of bases in a section of DNA on a chromosome: Some people have a different base at a given location
Classification of SNP by location • Coding region: Synonymous: mutation does not change amino acid. Non-synonymous: mutation changes amino acid seq. i.e. rare mutations that cause Mendelian diseases with allele frequencies below 1%. • Non-coding region: 5’ and 3’ UTR’s Introns Intervening Space
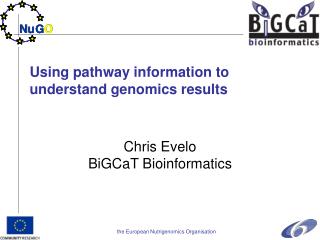
Affymetrix Scanner Illumina Bead Station GENOME-WIDE SNP ARRAYS SNP Array
SNP arrays have developed very rapidly: Size: 50K 100K 320K 550K 1000K 2.4M 5M Year: 2002 2004 2005 2006 2007 2008 2010 Offer the advantage of very dense coverage with over 5,000,000 data points across the genome. Costs $ Time (years)
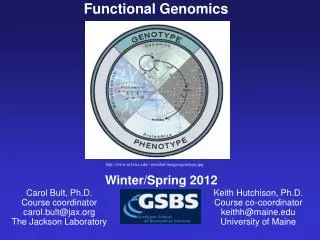
Genome-wide association study publications 600 500 400 Annual number of publications 300 200 100 1998 2000 2001 2002 2003 2004 2005 2006 2007 2008 1999 Years
The Trend & Applications of SNP markers Diseased Families Isolate Populations Case - Control cohorts Caes – Case studies Diseased Families Linkage Studies Candidate Regions Association studies Candidate Genes or genome-wide searches Positional Cloning Complex Diseases Drug Targets Diagnostic/Prognostic/Risk Markers Prevention Pharmacogenetics Candidate Genes Functional Studies Single Gene Disease Drug Targets/Diagnostics
Subject Ascertainment and Design Case-Control Design – most common Case selection – minimise phenotypic heterogeneity Can be constrained by financial or operational constraints or Focus on extreme and/or familial cases This could actually reduce power of detection
Control Selection • Optimal selection remains controversial • Some concerns over-stated (common controls do work WTCCC and Iceland) • Need to be aware of: • Selection bias • Misclassification bias • Population stratification
Other Case-Control Design Issues • Sample Size – the more the better • Population stratification and cryptic relatedness (potentially inflate type 1 errors) Matching of cases of controls is essential • Merits of Family-based and case-control association methods (good in reducing stratification problems but comes at a cost of reduced power). • Use of historical controls (storage and data acquisition problems)
Mapping Disease Genes microsatellites • Look for genetic linkage of disease to marker • Microsatellite markers are too widely spaced to identify individual genes. • There are common SNPs in every gene. • Need to identify those that are informative chromosome disease gene genes SNPs
Linkage Disequilibrium (LD) • LD occurs when a marker (microsatellite, SNP etc.) segregates with a disease gene. • Extremely important for mapping studies. • The likelihood of LD is a function of the distance between a marker and the gene of interest (ie. the closer a marker is to a disease gene the less likely a recombination event will occur).
Marker Selection and Assay Design • Marker selection: less of a problem due to increased marker density arrays and the dominance of companies involved in array production • DNA pooling: reduces costs but decreased power and less accuracy - becoming an irrelevant approach • Robustness of the genotyping data: HWE often used but imprecise for QC purposes. It can be indicative of an association if modestly present in cases
No association Stratification of relatedness Suggestive excess of strong association Compelling evidence of strong association Quantile-quantile plots Well defined Allele calling error Genotype call failure Biased estimates Signal Intensity plots Manhattan Plot
Validation and Replication • Importance of replication Technical Validation – re-analysis of original samples – make sure the genotypes called are as called Replication uses a NEW sample set that ideally includes both cases and controls
Optimal GWAS Design • GWAS on large sample set of Cases and Controls • Replication of the findings using a second assay platform (assay validation) • Replication of the study using a second set of cases and controls (do not need a 2nd GWAS study)
SNP success storiesCoronary Artery DiseaseColon CancerMultiple SclerosisBreast CancerCeliac DiseaseAutismProstate CancerOsteoporosisSystemic Lupus ErythromatosisSchizophreniarheumatoid arthritis
A GWAS for Pain • Must have a reliable measurement of pain (do not rely of self reporting) • Identify non-genetic causes of pain (personality and mood disorders) • Response to treatment • Age of onset • Nature of onset
Summary • Genetic studies required to identify new genetic factors • Case control studies for new biomarkers on risk • Case case studies for pharmacological response studies • Gene expression studies to understand mechanisms of pain • Proteomics required to understand the effect of genetic variation