Download
1 / 1
10 likes | 92 Views
KRAS MUTATION, CANCER RECURRENCE AND PATIENT SURVIVAL IN STAGE III COLON CANCER: FINDINGS FROM CALGB 89803

E N D
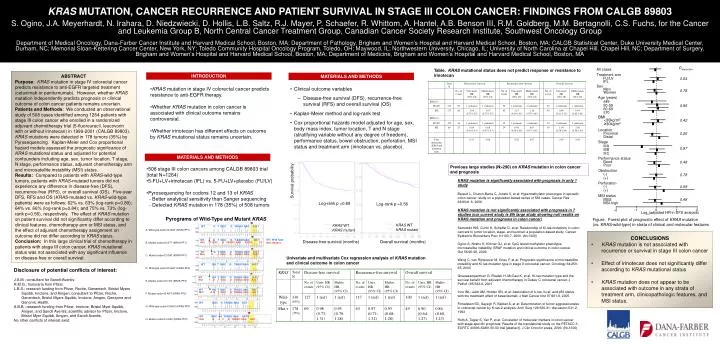
KRAS MUTATION, CANCER RECURRENCE AND PATIENT SURVIVAL IN STAGE III COLON CANCER: FINDINGS FROM CALGB 89803 S. Ogino, J.A. Meyerhardt, N. Irahara, D. Niedzwiecki, D. Hollis, L.B. Saltz, R.J. Mayer, P. Schaefer, R. Whittom, A. Hantel, A.B. Benson III, R.M. Goldberg, M.M. Bertagnolli, C.S. Fuchs, for the Cancer and Leukemia Group B, North Central Cancer Treatment Group, Canadian Cancer Society Research Institute, Southwest Oncology Group Department of Medical Oncology, Dana-Farber Cancer Institute and Harvard Medical School, Boston, MA; Department of Pathology, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA; CALGB Statistical Center, Duke University Medical Center, Durham, NC; Memorial Sloan-Kettering Cancer Center, New York, NY; Toledo Community Hospital Oncology Program, Toledo, OH; Maywood, IL; Northwestern University, Chicago, IL; University of North Carolina at Chapel Hill, Chapel Hill, NC; Department of Surgery, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA; Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA WT G T GGC G TAGGC AAG A G T WT G T GGC G T AGGCAAG AG T Mut TT GGC G TAGGC AAG A GTG CC WT G T GGC G TAGGC AAG A G T Mut A T GGC G TAGGC AAG A GT WT GG T GGC G TAGGCAAG A G T Pinteraction WT GG T GGC G TAGGC AAG A G T All cases Mut T G T GGC G TAGGC AAG A G T Treatment arm FU/LV 0.64 WT GG T GGC G TAGGC AAG AG T IFL Mut A G T GGC G TAGGC AAG AG T Sex Men 0.78 Women WT GGC G TAGGC AAG AGT Age (years) ≤49 50-59 0.95 WT GGC G TAGGC AAG AGTG 60-69 Mut G A C G TAGGC AAG AGT ≥70 BMI <30kg/m2 0.42 ≥30kg/m2 Location Proximal 0.26 Distal Stage IIIA 0.97 IIIB IIIC Performance status Good 0.48 Poor Obstruction (-) 0.78 (+) Perforation Survival probability (-) 0.59 (+) MSI status MSS 0.48 MSI-high -2 -1 0 1 2 Log-rank p =0.89 Log-rank p =0.56 Loge(adjusted HR in DFS analysis) KRAS WT KRAS mutant KRAS WT KRAS mutant Disease-free survival (months) Overall survival (months) Table. KRAS mutational status does not predict response or resistance to irinotecan ABSTRACT Purpose: KRAS mutation in stage IV colorectal cancer predicts resistance to anti-EGFR targeted treatment (cetuximab or panitumumab). However, whether KRAS mutation independently predicts prognosis or clinical outcome of colon cancer patients remains uncertain. Patients and Methods: We conducted an observational study of 508 cases identified among 1264 patients with stage III colon cancer who enrolled in a randomized adjuvant chemotherapy trial (5-fluorouracil, leucovorin with or without irinotecan) in 1999-2001 (CALGB 89803). KRAS mutations were detected in 178 tumors (35%) by Pyrosequencing. Kaplan-Meier and Cox proportional hazard models assessed the prognostic significance of KRAS mutational status and adjusted for potential confounders including age, sex, tumor location, T stage, N stage, performance status, adjuvant chemotherapy arm and microsatellite instability (MSI) status. Results: Compared to patients with KRAS-wild-type tumors, patients with KRAS-mutated tumors did not experience any difference in disease-free (DFS), recurrence-free (RFS), or overall survival (OS). Five-year DFS, RFS and OS (KRAS-mutated vs. KRAS-wild-type patients) were as follows: 62% vs. 63% (log-rank p=0.89); 64% vs. 66% (log-rank p=0.84); and 75% vs. 73% (log-rank p=0.56), respectively. The effect of KRAS mutation on patient survival did not significantly differ according to clinical features, chemotherapy arm or MSI status, and the effect of adjuvant chemotherapy assignment on outcome did not differ according to KRAS status. Conclusion: In this large clinical trial of chemotherapy in patients withstage III colon cancer, KRAS mutational status was not associated with any significant influence on disease-free or overall survival. INTRODUCTION MATERIALS AND METHODS • KRAS mutation in stage IV colorectal cancer predicts resistance to anti-EGFR therapy. • Whether KRAS mutation in colon cancer is associated with clinical outcome remains controversial. • Whether irinotecan has different effects on outcome by KRAS mutational status remains uncertain. • Clinical outcome variables • Disease-free survival (DFS), recurrence-free survival (RFS) and overall survival (OS) • Kaplan-Meier method and log-rank test • Cox proportional hazards model adjusted for age, sex, body mass index, tumor location, T and N stage (stratifying variable without any degree of freedom), performance status, bowel obstruction, perforation, MSI status and treatment arm (irinotecan vs. placebo). MATERIALS AND METHODS Previous large studies (N>290) on KRAS mutation in colon cancer and prognosis • 508 stage III colon cancers among CALGB 89803 trial (total N=1264) • 5-FU+LV+irinotecan (IFL) vs. 5-FU+LV+placebo (FU/LV) • Pyrosequencing for codons 12 and 13 of KRAS • - Better analytical sensitivity than Sanger sequencing • - Detected KRAS mutation in 178 (35%) of 508 tumors KRAS mutation is significantly associated with prognosis in only 1 study Barault L, Charon-Barra C, Jooste V, et al: Hypermethylator phenotype in sporadic colon cancer: study on a population-based series of 582 cases. Cancer Res 68:8541-6, 2008 KRAS mutation is not significantly associated with prognosis in 7 studies (our current study is 8th large study showing null results on KRAS mutation and prognosis in colon cancer) Samowitz WS, Curtin K, Schaffer D, et al: Relationship of Ki-ras mutations in colon cancers to tumor location, stage, and survival: a population-based study. Cancer Epidemiol Biomarkers Prev 9:1193-7, 2000. (N>1300) Ogino S, Nosho K, Kirkner GJ, et al: CpG island methylator phenotype, microsatellite instability, BRAF mutation and clinical outcome in colon cancer. Gut 58:90-96, 2009. Wang C, van Rijnsoever M, Grieu F, et al: Prognostic significance of microsatellite instability and Ki-ras mutation type in stage II colorectal cancer. Oncology 64:259-65, 2003 Gnanasampanthan G, Elsaleh H, McCaul K, et al: Ki-ras mutation type and the survival benefit from adjuvant chemotherapy in Dukes' C colorectal cancer. J Pathol 195:543-8, 2001 Ince WL, Jubb AM, Holden SN, et al: Association of k-ras, b-raf, and p53 status with the treatment effect of bevacizumab. J Natl Cancer Inst 97:981-9, 2005 Finkelstein SD, Sayegh R, Bakker A, et al: Determination of tumor aggressiveness in colorectal cancer by K-ras-2 analysis. Arch Surg 128:526-31; discussion 531-2, 1993 Roth A, Tejpar S, Yan P, et al: Correlation of molecular markers in colon cancer with stage-specific prognosis: Results of the translational study on the PETACC 3 - EORTC 40993-SAKK 60-00 trial [abstract]. J Clin Oncol:in press, 2009. (N>1300) Pyrograms of Wild-Type and Mutant KRAS Figure. Forest plot of prognostic effect of KRAS mutation (vs. KRAS-wild-type) in strata of clinical and molecular features A. Wild-type codon12 GGT (KRAS-PF1) • CONCLUSIONS • KRAS mutation is not associated with recurrence or survival in stage III colon cancer • Effect of irinotecan does not significantly differ according to KRAS mutational status • KRAS mutation does not appear to be associated with outcome in any strata of treatment arm, clinicopathologic features, and MSI status. WT; Wild Type Mut; Mutant B. Mutant codon12 GTT (KRAS-PF1) C. Mutant codon12 GAT (KRAS-PF1) Univariate and multivariate Cox regression analysis of KRAS mutation and clinical outcome in colon cancer D. Wild-type codon12 GGT (KRAS-PF2) Disclosure of potential conflicts of interest: J.A.M.; consultant for Sanofi-Aventis R.M.G.; honoraria from Pfizer. L.B.S.; research funding from Pfizer, Roche, Genentech, Bristol Myers Squibb, Imclone, and Amgen; consultant to Pfizer, Roche, Genentech, Bristol Myers Squibb, Imclone, Amgen, Genzyme and Genomic Health. A.B.B.; research funding from Pfizer, Imclone, Bristol Myer Squibb, Amgen, and Sanofi Aventis; scientific advisor for Pfizer, Imclone, Bristol Myer Squibb, Amgen, and Sanofi Aventis. No other conflicts of interest exist. E. Mutant codon12 TGT (KRAS-PF2) F. Mutant codon12 AGT (KRAS-PF2) G. Wild-type codon13 GAC (KRAS-PF3) H. Mutant codon13 GAC (KRAS-PF3)



















