Download
1 / 1
10 likes | 318 Views
Poster #710 13 th Conference on Retroviruses and Opportunistic Infections February 5 – 8, 2006 Denver, CO, USA. Adequate Lopinavir (LPV) Exposure Achieved with a Higher Dose During the 3rd Trimester of Pregnancy. Mark Mirochnick, MD 91 East Concord St Boston, MA 02118

E N D
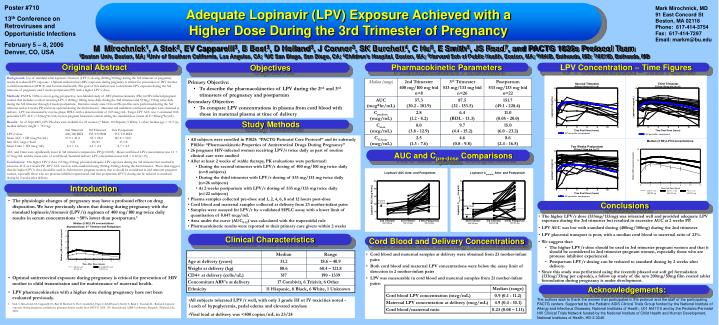
Poster #710 13th Conference on Retroviruses and Opportunistic Infections February 5 – 8, 2006 Denver, CO, USA Adequate Lopinavir (LPV) Exposure Achieved with a Higher Dose During the 3rd Trimester of Pregnancy Mark Mirochnick, MD 91 East Concord St Boston, MA 02118 Phone: 617-414-3754 Fax: 617-414-7297 Email: markm@bu.edu M Mirochnick1, A Stek2, EV Capparelli3, B Best3, D Holland3, J Connor3, SK Burchett4, C Hu5, E Smith6, JS Read7, and PACTG 1026s Protocol Team 1Boston Univ, Boston, MA; 2Univ of Southern California, Los Angeles, CA; 3UC San Diego, San Diego, CA; 4Children’s Hospital, Boston, MA; 5Harvard Sch of Public Health, Boston, MA; 6NIAID, Bethesda, MD; 7NICHD, Bethesda, MD OriginalAbstract Objectives Pharmacokinetic Parameters LPV Concentration – Time Figures Background: Use of standard adult lopinavir/ritonavir (LPV/r) dosing (400mg/100mg) during the 3rd trimester of pregnancy results in reduced LPV exposure. Optimal antiretroviral (ARV) exposure during pregnancy is critical for prevention of HIV mother to child transmission (MTCT) and for maternal health. The goal of this analysis was to determine LPV exposure during the 3rd trimester of pregnancy and 2 weeks postpartum (PP) with a higher LPV/r dose. Methods: PACTG 1026s is an on-going, prospective, non-blinded study of ARV pharmacokinetics (PK) in HIV-infected pregnant women that includes a cohort receiving LPV/r 400mg/100mg twice daily during the 2nd trimester and 533mg/133mg twice daily during the 3rd trimester through 2 weeks postpartum. Intensive steady-state 12-hour PK profiles were performed during the 3rd trimester and at 2 weeks PP, and were optional during the 2nd trimester. Maternal and umbilical cord blood samples were obtained at delivery. LPV was measured by reverse-phase HPLC with a detection limit of 0.05 mcg/mL. Target LPV AUC was > estimated 10th percentile LPV AUC (>52mcg*hr/mL) in non-pregnant historical controls taking the standard dose (mean AUC=80mcg*hr/mL). Results: As of Sept 2005, LPV PK data were available for 23 women (7 Black, 10 Hispanic, 5 White, 1 other; median age = 31.9 yrs, median delivery weight = 79.1 kg). 2nd Trimester 3rd Trimester 2wk Postpartum LPV/r dose 400/100 BID 533/133 BID 533/133 BID Mean AUC + SD (mcg*hr/mL) 57.9 + 21.6 85 + 28.2 145.8 + 50.0 Met AUC target/Total 5/8 20/23 17/18 Mean Cmin + SD (mcg/mL) 2.4 + 1.6 4.5 + 2.4 8.7 + 4.5 AUC and Cmin were significantly lower in 3rd trimester compared to PP (p<0.005). Mean cord blood LPV concentration was 1.1 + 0.7 mcg/mL and the mean ratio of cord blood/maternal delivery LPV concentration was 0.24 + 0.12 (n=15). Conclusions: The higher LPV/r dose (533mg/133mg) provided adequate LPV exposure during the 3rd trimester but resulted in excessive AUC at 2 weeks PP. LPV AUC was low with standard dosing (400mg/100mg) during the 2nd trimester. These data suggest that the higher LPV/r dose should be used in 3rd trimester pregnant women, that it should be considered in 2nd trimester pregnant women, especially those who are protease inhibitor experienced, and that postpartum LPV/r dosing can be reduced to standard dosing by 2 weeks after delivery. • Primary Objective: • To describe the pharmacokinetics of LPV during the 2nd and 3rd trimesters of pregnancy and postpartum • Secondary Objective: • To compare LPV concentrations in plasma from cord blood with those in maternal plasma at time of delivery k Study Methods • All subjects were enrolled in P1025: “PACTG Perinatal Core Protocol” and its substudy P1026s: “Pharmacokinetic Properties of Antiretroviral Drugs During Pregnancy” • 26 pregnant HIV-infected women receiving LPV/r twice daily as part of routine clinical care were studied • After at least 2 weeks of stable therapy, PK evaluations were performed: • During the second trimester with LPV/r dosing of 400 mg/100 mg twice daily (n=8 subjects) • During the third trimester with LPV/r dosing of 533 mg/133 mg twice daily (n=26 subjects) • At 2 weeks postpartum with LPV/r dosing of 533 mg/133 mg twice daily (n=22 subjects) • Plasma samples collected pre-dose and 1, 2, 4, 6, 8 and 12 hours post-dose • Cord blood and maternal samples collected at delivery from 23 mother-infant pairs • Samples were assayed for LPV/r by a validated HPLC assay with a lower limit of quantitation of 0.047 mcg/mL • Area under the curve (AUC0-12) was calculated with the trapezoidal rule • Pharmacokinetic results were reported to their primary care givers within 2 weeks AUC and Cpre-dose Comparisons Introduction • The physiologic changes of pregnancy may have a profound effect on drug disposition. We have previously shown that dosing during pregnancy with the standard lopinavir/ritonavir (LPV/r) regimen of 400 mg/100 mg twice daily results in serum concentrations ~50% lower than postpartum.1 • Optimal antiretroviral exposure during pregnancy is critical for prevention of HIV mother to child transmission and for maintenance of maternal health. • LPV pharmacokinetics with a higher dose during pregnancy have not been evaluated previously. • Stek A, Mirochnick M, Capparelli1 E, Best B, Burchett S, Hu C, Gardella J, Elgie C, Schiffhauer J, Smith E, Read J, Tuomala R.. Reduced lopinavir exposure during pregnancy: preliminary pharmacokinetic results from PACTG 1026. XV International AIDS Conference, Bangkok, Thailand, July, 2004. Conclusions • The higher LPV/r dose (533mg/133mg) was tolerated well and provided adequate LPV exposure during the 3rd trimester but resulted in excessive AUC at 2 weeks PP. • LPV AUC was low with standard dosing (400mg/100mg) during the 2nd trimester. • LPV placental transport is poor, with a median cord blood to maternal ratio of 23%. • We suggest that: • The higher LPV/r dose should be used in 3rd trimester pregnant women and that it should be considered in 2nd trimester pregnant women, especially those who are protease inhibitor experienced. • Postpartum LPV/r dosing can be reduced to standard dosing by 2 weeks after delivery. • Since this study was performed using the recently phased out soft gel formulation (133mg/33mg per capsule), a follow up study of the new 200mg/50mg film coated tablet formulation during pregnancy is under development. Clinical Characteristics Cord Blood and Delivery Concentrations • Cord blood and maternal samples at delivery were obtained from 23 mother-infant pairs • Both cord blood and maternal LPV concentrations were below the assay limit of detection in 2 mother-infant pairs • LPV was measurable in cord blood and maternal samples from 21 mother-infant pairs: Acknowledgements: • All subjects tolerated LPV/r well, with only 3 grade III or IV toxicities noted - 1 each of hypoglycemia, pedal edema and elevated amylase • Viral load at delivery was <400 copies/mL in 23/24 The authors wish to thank the women that participated in the protocol and the staff of the participating PACTG centers. Supported by the Pediatric AIDS Clinical Trials Group funded by the National Institute of Allergy and Infectious Diseases, National Institutes of Health, U01 AI41110 and by the Pediatric/Perinatal HIV Clinical Trials Network funded by the National Institute of Child Health and Human Development, National Institutes of Health, HD-3-3345.