Download
1 / 45
450 likes | 533 Views
The Respiratory System. Functions. Ventilation (inhalation and exhalation) Gas exchange (alveoli blood & blood tissues ) Additional functions: Sound production Enables “non-breathing” air movements (sneezing, coughing, laughing etc.). Characteristics.

E N D
Functions • Ventilation (inhalation and exhalation) • Gas exchange (alveoli blood & blood tissues) • Additional functions: • Sound production • Enables “non-breathing” air movements (sneezing, coughing, laughing etc.)
Characteristics • Usually 14-20 breaths/minute • About 450 ml per breath at rest or up to 100 L/minute during exercise • Breathing is automatic and unconscious but one can hold his/her breath up to a certain point • If no air for: • 4-5 minutes: loss of consciousness • 7-8 minutes = brain damage • 10 minutes = impending death
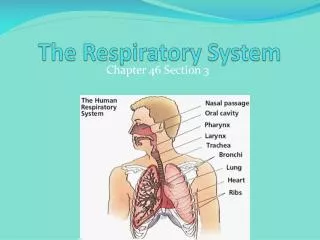
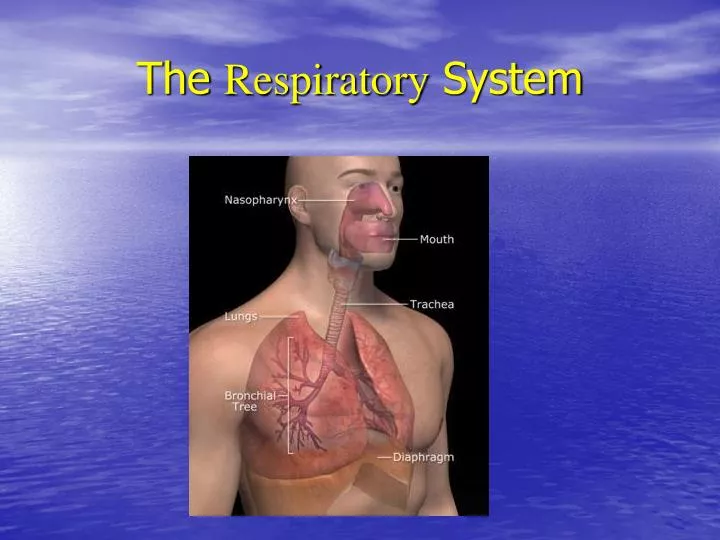
Ventilation • Movements of air in and out of the lungs • Made possible by the presence of the respiratory system: • upper airway: nose to pharynx • Lower airway: larynx to alveoli
Upper respiratory system Lower respiratory system
Nose Nasopharynx Oropharynx Upper airway
Primary air entrance Number of cartilages Lateral cartilage (bridge) Alar cartilages (lesser & greater nostrils) Septal cartilage (anterior portion of the septum) Also includes paired nasal bones Supported byvomer& perpendicular plate of theethmoid bone Support the septum (what divides nasal opening into left & right halves…each side =nasal fossa) Nose
Nasal Cavity - roles • Breathing: due to conchae- air is spinned around • “filter” air by embedding particulate matter into mucus • “warm” air (places capillary bed close to the surface) • Moisten air • olfaction” by spinning olfactory matter up against inferior side of ethmoid bone (olfactory bulb) • Also acts as resonating chamber for your voice
Tissues Stratified squamous epithelium Pseudostratified columnar epithelium Presence of goblet cells in epithelium: secrete mucus moisten air and trap dust paticles
Paired air spaces in the anterior skull: Maxillary, frontal, sphenoidal & ethmoidal Decrease skull weight Help with sound resonance (both for hearing and voice) Paranasal Sinuses
Funnel-shaped “tube” 15cm long Connects nasal & oral cavities to larynx & esophagus One set of tonsils are located in the pharynx pharyngeal tonsils or adenoids Act to sample incoming pathogens etc. and provide first-line immunity exposure Nasopharynx
Uvula: lower or caudal end of the nasopharynx Can also see pharyngeal tonsils (adenoids) lateral to the uvula Eustuchian or auditory tubes open in the back of the nasopharynx Swallowing: uvula & soft palate will be elevated to block nasal cavity to keep bolus from entering the nasal cavity Why you inspire before swallowing Nasopharynx
middle region of the pharynx Between soft palate & hyoid bone Imagine the back of your tongue-just above the laryngeal prominence Region where BOTH air & bolus pass Palatine tonsils located on posterior wall (on each side) Lingual tonsils located on the base of the tongue (more anterior) Oropharynx
Laryngopharynx: distal region of the pharynx From hyoid bone – esophagus/larynx Where the bolus or air is directed to the correct passagway Air & bolus (food) must CROSS in the three regions of the pharynx (particularly in the oropharynx and laryngopharynx region risk of choking. Laryngopharynx
Lower airway • Larynx • Trachea • Bronchial tree • Alveoli
Larynx • Functions: • Prevent bolus from entering trachea & lungs • Produce sound • Laryngeal muscles • Extrinsic laryngeal muscles help to draw up larynx when swallowing bolus (to fold epiglottis over glottis) • Intrinsic laryngeal muscles control tension of the vocal cords • Control length, tension & position of the vocal cords/membrane • The thicker & longer the membrane/cords, the deeper the sound
Larynx • 9 separate cartilage units that form the “voice box” • Three main “single” cartilages: • Thyroid cartilage – (Adam’s apple in males) • Cricoid cartilage – ring at the base of the thyroid cartilage • Epiglottis: connective tissue framed by hyaline cartilage • Acts as a levered flap during swallowing: larynx is drawn cranially by extrinsic muscles and levers the epiglottis against hyoid bone down over glottis • Three smaller pairs of cartilages • Arytenoid • Cuneiform • Corniculate cartilages
Airway obstruction: if the object is large enough to be lodged within the larynx/trachea, it will usually be found in the region of the cricoid cartilage. The cricoid & thyroid cartilages have the smallest internal diameter of all the laryngeal structures.
Larynx • Vocal cords • Connective tissue stretched across the larynx “bore” from thyroid cartilage – arytenoid cartilage • Vestibular folds act to support the vocal cords & keep them moist
“windpipe” organ Semi-rigid structure connecting larynx to primary bronchii 16-20 “C”-shaped “tracheal cartilages” C-shape allows esophageal expansion during swallowing Carina (where primary bronchii branches can be found) = landmark for intubation Lined by pseudostratified columnar epithelium (ciliated) Recall nasal conchae Trachea
Epithelium: ciliated pseudocolumnar epithelium (to eliminate dust particles Mid layer: hyaline cartilage (to prevent collapse) Wall of trachea and bronchi
From the carina: Primary bronchii – going toward right and left lungs Near sternal angle of the manubrium Right bronchii is more “vertical” and wider than left If you aspirate a liquid or particle, it will likely end up in the right bronchii Secondary or lobar bronchi Tertiary or segmental bronchii Bronchioles after further division Bronchial Tree
connection to the functional region of respiratory tract No longer ringed by cartilage smooth muscle in the wall Asthma = allergic constriction of the smooth muscles surrounding the bronchiole passages Terminal bronchioles connect to the respiratory bronchioles, which finally enter the alveolar ducts Bronchioles
Final destination for inspired air flow Bear in mind that inspired/expired air is rarely “fully” exchanged Almost 85% of the volume of inspired air remains within the respiratory tract during the next cycle of expiration/inspiration Region of gas exchange 350 million alveoli/lung ( 70 M2) “simple” squamous epithelium “air-blood” barrier = 1 cell thick + basement membrane + capillary endothelium Pulmonary Alveoli
Pulmonary Alveoli • 2 types of alveolar cells: • Type I = squamous epithelial cells • Type II = “surfactant” secreting cells • Surfactant = mixture of lipids & proteins (SP-A, SPB & SP-C) • Goal is to reduce surface tension within the alveolus (prevents alveolar collapse) • Decreases the effort to breathe & keep alveolar sacs “open” • Presence of small amount of elastic connective tissue between alveoli and capillaries promote lung tissue recoil and allow for passive exhalation
Because of frequent bursts of high pressure in the alveoli, the alveolar tissue get stretched alveoli fuse into a large sphere less surface for gas exchanges, scar tissue formation Common in chronic lung diseases (COPD) Emphysema
Surfactant • Remember that the surface of the alveoli is covered with a watery fluid very high surface tension • Ex: The surfaces of a wet plastic bag will stick to each other • the walls of the alveoli tend to stick together difficult to re-open the alveoli) • Surfactant secreted by Type II alveolar cells decrease this surface tension • Permits more effective gas exchange • Also permits alveolar expansion/contraction with less risk of “vacuum collapse”
Surfactants begin to be secreted around the 7th month of pregancy Premature babies lack surfactant Hyaline membrane disease, deadly if untreated “surfactant replacement therapy” has vastly improved survival rates among premies (up to 95% from 5% for 6-6.5 month old premies) Surfactant
Paired organs separated by mediastinum 4 surfaces: Mediastinal/medial with the hilum: point of entry of the vessels and bronchi) Base (diaphragm side) Apex (cranial side) “costal surface” = surface facing costals Lungs not identical: L-lung has 2 distinct lobes R-lung has 3 lobes Lungs
Pleurae • Parietal pleuraover each lung (physically adhered to internal layer of thorax) • Visceral pleura intimate to each lung • Between each layer of pleurae = serous fluid • Lubricant prevents friction • Promotes “negative pressure” (vacuum)
Collapse of the lung due to entry of air into the pleural cavity Entry can be from outside, due to stabbing, gunshot wound, broken ribs or from inside due to ruptured alveoli Do not confuse pneumothorax with atelectasis, which is collapsed alveoli (due to inadequate breathing depth) Pneumothorax
Pulmonary Ventilation (breathing) • Inspiration: due to contraction of : • diaphragm (phrenic n.) • intercostal muscles (both external & internal, costal nerves) • Expanding the thorax reduces pressure within the lungs (you don’t “suck in air”…you “vacuum” it) • Expiration: relaxation of muscles • Recoil of elastic fibers in tissue • Allows costovertebral joint to return to original position • As lungs constrict, surfactant prevents alveolar collapse
Non-respiratory Air Movements • Coughing: deep inspiration, closure of the glottis, followed by strong expulsion that forces open the glottis • Sneeze= air exits via nasal cavity rather than oral cavity • Yawn= deep inspiration, pause, sudden expiration • Laugh= deep inspiration followed by sudden & rapid expirations • Cryingis very similar, but glottis remains open the entire time…why you often choke when you cry • Hiccup= spastic diaphragm contractions (irritated phrenic n.)
Cleft palate & cleft lip • During fetal development, L & R sides of the oral cavity failed to fuse difficulty breathing and eating • Both can be effectively repaired with cosmetic surgery
Smoking and lung cancer Effects of smoking • Cancer of the mouth
Black lung due to coal exposure Cystic fibrosis: a genetic defect of chloride ion channels which promote formation of thick mucus Respiratory Pathophysiology