Download
1 / 34
340 likes | 658 Views
Osteoarthritis. Randa Mahmoud Al-HarizyInternal Medicine departmentFaculty of Medicine, Cairo University. OA is a group of diseases and mechanical abnormalities entailing degradation of joints, including articular cartilage and the subchondral bone next to it OA is derived from the Greek word

E N D
2. Osteoarthritis Randa Mahmoud Al-Harizy
Internal Medicine department
Faculty of Medicine, Cairo University
3. OA is a group of diseases and mechanical abnormalities entailing degradation of joints, including articular cartilage and the subchondral bone next to it
OA is derived from the Greek word �ostoe�, meaning �of the bone�, �arthro�, meaning �joint�, and �itis�, meaning inflammation
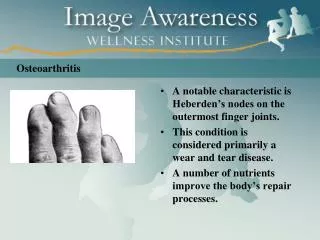
4. There is no simple definition of OA as it requires consideration of three overlapping areas - pathological changes, radiological features and clinical consequences. Pathologically, there is an alteration in cartilage structure, radiologically there are osteophytes and joint space narrowing, and clinically some patients complain of pain and disability.
6. Osteoarthritis is the most common type of arthritis.
The prevalence increases with age
80% of people over 60 years will have some radiological evidence of it, although only 60% of those will show symptoms.
7. O.A.
Women over 55 years are affected more commonly than are men of a similar age.
There is a familial pattern of inheritance
The resulting disabilities have major socio-economic resource implications, particularly in the developed world.
9. In OA, a variety of potential forces; hereditary, developmental, metabolic and mechanical may initiate processes leading to loss of cartilage.
Subchondral bone may be exposed and damaged, with regrowth leading to a proliferation of ivory-like, dense, reactive bone in central areas of cartilage loss, a process called eburnation.
The patient experiences pain upon weight bearing
Due to decreased movement from pain, regional muscles may atrophy and ligaments may become more lax
11.
Obesity
Heredity
Gender
Hypermobility
Osteoporosis
Trauma
Congenital joint dysplasia
Occupation
Sport
12. Primary OA: No known cause
Secondary OA
Pre-existing joint damage:���RA,�Gout,�Seronegative spondyloarthropathy,�Septic arthritis,�Paget's disease, Avascular necrosis, e.g. corticosteroid therapy�
Metabolic disease:�Chondrocalcinosis,�Hereditary haemochromatosis,�Acromegaly�
Systemic diseases:�Haemophilia- recurrent haemarthrosis,�Haemoglobinopathies, e.g. sickle cell disease,�Neuropathies
13. CLINICAL PICTURE
OA commonly affects the hands, feet, spine and the large weight bearing joints such as hips and knees
Symptoms
Joint pain
Joint gelling (stiffening and pain after immobility)
Joint instability
Loss of function.
14. CLINICAL PICTURE
Signs
Joint tenderness
Crepitus on movement
Limitation of range of movement
Joint instability
Joint effusion and variable levels of inflammation
Bony swelling
Wasting of muscles.
16. DIAGNOSIS Investigations in OA
Blood tests. There is no specific test; the ESR and CRP are normal. Rheumatoid factor and antinuclear antibodies are negative.
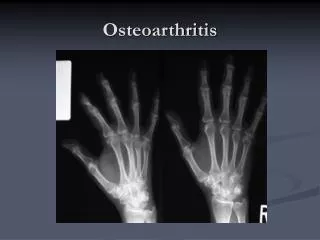
X-rays are abnormal only when the damage is advanced.
MRI demonstrates early cartilage and subchondral bone changes.
Arthroscopy reveals early fissuring and surface erosion of the cartilage.
19. TREATMENT Generally speaking, the process of clinically detectable osteoarthritis is irreversible, and typical treatment consists of medication or other interventions that can reduce the pain of OA and thereby improve the function of the joint.
20. CONSERVATIVE CARE Weight control
Appropriate rest and Exercise
Physical therapies
Occupational therapies
21. DIETARY TREATMENT
Glucoseamine, chondroitin sulphate, antioxidants, others�
SPECIFIC MEDICATIONS
Paracetamol
NSAIDs
COX-2 selective inhibitors
Corticosteroids
22. OTHERS Implantation of chondrocytes
Local injection of hyaluronic acid
Topical treatment
Surgical treatment
Acupuncture
23. Crystal Deposition Disease GOUT
Definition:
Gout is a disease which is characterized by tissue deposition of monosodium urate crystals (MSU) due to hyperuricaemia that results in:
Gouty arthritis
Tophi
Gouty nephropathy
Uric acid nephrolithiasis
24. ETIOLOGY 1- Overproduction of urate:
Endogenous:
Hyperactivity of phosphoribosylpyrophosphate (PRPP) synthetase
Partial deficiency of hypoxanthine guanine phospho-ribosyltransferase (HGPRT)
Myeloproliferative and lymphoproliferative disorders
Hemolysis
Psoriasis
Exogenous:
Excess dietary purine consumption: meat, liver, kidney, sea food, legumes, mushrooms
25. Underexcretion of Urate Renal disease
Lead intoxication
Hyperparathyroidism
Hypothyroidism
Drugs:
Low dose aspirin
Diuretics
Ethambutol
Pyrazinamide
Cyclosporine
Alcohol
26. CLINICAL PICTURE 1- Asymptomatic hyperuricemia
2- Acute gouty arthritis:
- precipitating factors: excess dietary purines, alcohol, drugs, surgery, trauma, dehydration
- typically affected joints of lower limb more commonly than that of upper limb; the first metatarsophalangeal joint of big toe, the tarsals, ankles, heels, knees, wrists and fingers in a descending order
Presentation: early in the course of the disease is monoarticular, of acute onset, often during night. The affected joint is exquisitely painful, warm, red and swollen. Subsequent attacks become polyarticular and persist longer
27. CLINICAL PICTURE 3- Intercritical gout: asymptomatic intervals between the acute attacks
4- Chronic tophaceous gout: development of subcutaneous nodules of deposits of monosodium urate crystals
28. INVESTIGATIONS Serum level of uric acid may be elevated
Synovial fluid analysis for:
Cells: 25.000 � 100.000 leukocytes/mm3
Polarized microscopy of the synovial fluid reveals the typical needle shaped negative birefringent crystals
Radiology: soft tissue swelling, punched out bone erosions
29. TREATMENT During the acute attack:
NSAIDs: indomethacin , Colchicine, ACTH, Intraarticular steroids, systemic corticosteroids
Treatment of chronic tophaceous gout
Xanthine oxidase inhibitor (allopurinol)
Uricosuric drugs: probenecid
Diet control
30. PSEUDOGOUT Definition
Pseudogout is an inflammatory arthropathy resulting from deposition of calcium pyrophosphate dihydrate crystals (CPPD) in and around joints that results in calcification of articular cartilage (chondrocalcinosis)
31. Conditions associated with pseudogout Hyperparathyroidism
Haemochromatosis
Osteoarthritis
Hypothyrodism
Neuropathic arthropathy
Idiopathic
Familial
32. Clinical picture Acute pseudogout:
Acute monoarthritis especially affecting knee, ankle, wrist or shoulder. Surgical procedures and acute medical illness may precipitate the attack
Chronic pseudogout:
Presenting as osteoarthritis but distinguished from it by the involvement of atypical joints as wrists and metacarpophalangeal joints
33. INVESTIGATIONS SYNOVIAL FLUID ANALYSIS FOR:
Cells 25.000 � 100.000 leukocytes/mm3
Polarized microscopy of the synovial fluid reveals the typical rhomboid shaped positive birefringent crystals
RADIOLOGY
Chondrocalcinosis with evidence of calcification of fibrocartilage as menisci, symphisis pubis and triangular cartilage of the wrist
34. TREATMENT NSAIDs
Joint aspiration
Intraarticular injection of steroids