Download
1 / 14
140 likes | 154 Views
Learn steps to implement Race Equality in PCT through communication, executive commitment, staff workshops, and linking to business plans. Understand different organizational maturity levels and competency stages for successful integration. Identify success factors, like leadership and ongoing support, and address challenges like resistance to change. Dive deep into adopter characteristics in NHS organizations and develop a clear vision and strategy for diversity integration. Follow expert insights for sustainable progress.

E N D
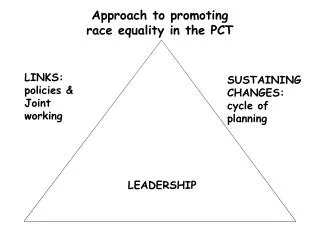
Making Race Equality stick in a PCT • Our commission - re-drafting the scheme • building involvement: communication and connection • Senior Executive commitment • Staff workshops • Linking to corporate objectives and business plans • limited priorities, clear commitments, lead responsibilities Su Kingsley, STRAD Consulting
2: Figure A: PCT Dimensions Finding their way Naive Astute Organisational Maturity Swamped External Challenge Structural Chaos Dinosaurs Struggling Phoenix Surviving New Borns
Mainstreaming at different levels Purpose Identity What do you want to achieve - Maturity Values & beliefs Capability Systems and processes in place to deliver - Structure Behaviour Impact of the external environment - Challenge Environment Su Kingsley, STRAD Consulting
Steps to competence Unconscious competence practice Conscious competence process content Conscious incompetence Unconscious incompetence Su Kingsley, STRAD Consulting
Learning model: Implications for implementing RRAA Conscious incompetence Conscious competence Unconscious incompetence Unconscious competence Will implement RRAA if told how and what to do - unlikely to learn or make further connections Will work hard to set up processes for RRAA, but unlikely to integrate into strategic or operational plans Proactive in raising and reviewing equitable access, appropriate services delivery and community consultations Collects & uses monitoring data Invests in staff training Clear vision & strategy for how diversity is integrated throughout the organisation’s processes and people Data systems support integration Community is fully involved in service planning & development Su Kingsley, STRAD Consulting
Not rocket science… …more marathon running Su Kingsley, STRAD Consulting
Learning model - where are most NHS organisations? ‘Conscious incompetence’ Working on competence - ‘conscious competence’ Unconscious incompetence Becoming competent Late majority Early majority Early Adopters Innovators Laggards Adoption curve descriptions Su Kingsley, STRAD Consulting
Applying adopter characteristics to NHS organisations 2nd/3rd wave developments request guidance on implementation join established developments will seek to apply ‘good practice’ Don’t initiate developments wait for circular/guidance compliant - follow instructions strongly influenced by peers need support - likely to implement form rather than spirit Early members of collaboratives participate in pilot programmes Leaders & members of learning partnerships Potential for good practice Resistant to change until instructed will not introduce new practices unless they are made a requirement require heavy performance management do not respond to good examples Participate in national pilots linked to DoH associated with research centres ‘transformational project’ leaders 2.5% 13.5% 34% 34% 16% Innovators Early Adopters Early majority Late majority Laggards Su Kingsley, STRAD Consulting
Success factors • Leadership • Applying corporate values • Senior diversity specialist • On-going support and training • Systematic integration into all business functions Su Kingsley, STRAD Consulting
Naive Finding their way Astute No vision, framework or plan Lacks systems & procedures -Survive by following instructions unclear of local needs Risk management not on the agenda Systems & processes at early stage Struggling to develop partnerships Culturally Risk averse Link local health needs into national priorities Clear vision - prioritise national and local agenda Delivery systems in place Able to manage risks Focused on meeting local health needs Good at sustaining partnerships Dimension 1: “Organisational maturity” Implications for implementing RRAA Require instructions - will implement RRAA if it is a low risk ‘must do’ Will only do what they perceive as being a national requirement Need to be shown how to connect race equality with other aspects of business Need to see RRAA as explicit national priority Encouraged by being shown benefits of RRAA implementation Will follow lead of influencers, examples of good practice Opportunistic - may seek resource for implementation Need to understand how RRAA helps meet local health needs May be innovative - potential source of good practice Will be influenced by lead of significant others Su Kingsley, STRAD Consulting
Dinosaurs Phoenix New Borns PCT welded onto structure of former Community Health Services Trust Not yet thinking through new role(s) - struggling with commissioning Inherited problems - policies, practice, premises Regurgitated CHS policies & procedures Built from predecessor Primary Care group(s) - reinventing everything! Lacks history of experience as former organisation - little former development to build on Lacks skills & capacity - also struggling with commissioning role No organisational history - context of total change throughout local health economy Leadership recently appointed No organisational memory Lack of systems and procedures Dimension 2: “Structural Chaos” Implications for implementing RRAA Likely to take procedural approach May have previous policies and structures to rely on Will be seen to comply - letter more than spirit Need to be pushed to implement RRAA Need to be shown benefits Need information to involve stakeholders Opportunity to integrate RRAA into planning and systems development Need to be stimulated to recognise opportunities to implement RRAA Su Kingsley, STRAD Consulting
Swamped Struggling Surviving Serious financial constraints High deprivation indices High staff and population mobility pressure to address race equality Balancing the books with difficulty Adequate local health economy infrastructure No major financial challenge Stable population Staff retention good Involved public Dimension 3: “External Challenge” Implications for implementing RRAA Will need to see specific benefits of implementing RRAA in terms of the rest of the ‘must do’ agenda Need to be convinced of need for population data and encouraged to use it Attention likely to be focused on national priorities Will implement RRAA if it is identified on the list of ‘must do’ requirements; difficult in mainstreaming Potential to work effectively within local health economy Have capacity to invest in systems to deliver race equality: e.g. ability to collect & use ethnicity data Unlikely to be under pressure for change locally - need external stimulus to initiate action Su Kingsley, STRAD Consulting
Opportunities for integration….. • Business plan, Corporate Objectives • Local Development Plan • Service and Financial Framework (SaFF) • Clinical governance framework • National Service Framework implementation plans • Health Improvement Programme • IWL - workforce plan, retention and recruitment strategy • Patient and Public involvement Su Kingsley, STRAD Consulting
Core principles of our approach • Builds on your existing work • Links to mainstream targets and objectives • Action focused • Sets achievable priorities • Reviewable Su Kingsley, STRAD Consulting