Download

1 / 61
770 likes | 911 Views
NAFLD. 1)Epidemiology, clinical features, and diagnosis of nonalcoholic fatty liver disease in adults Dr.mousavi -Abadan- Khordad 1397.

E N D
NAFLD 1)Epidemiology, clinical features, and diagnosis of nonalcoholic fatty liver disease in adults Dr.mousavi-Abadan-Khordad 1397
DEFINITIONS — Patients with nonalcoholic fatty liver disease (NAFLD) have hepatic steatosis, with or without inflammation and fibrosis. In addition, no secondary causes of hepatic steatosis are present. NAFLD is subdivided into: • Nonalcoholic fatty liver (NAFL) • Nonalcoholic steatohepatitis (NASH).
EPIDEMIOLOGY: Prevalence: The most common liver disorder in Western industrialized countries . • Prevalence of NAFLD of 10 to 46 percent • Most biopsy-based studies reporting a prevalence of NASH of 3 to 5 percent . • Worldwide, NAFLD has a reported prevalence of 6 to 35 percent (median 20 percent).
Between 1988 and 1994, the prevalence of NAFLD was 5.5 percent • between 1999 and 2004 it was 9.8 percent • between 2005 and 2008 it was 11 percen • Over the same three time periods, there were also increases in the rates of other components of the metabolic syndrome (table 1), including obesity (22, 30, and 33 percent, respectively), type 2 diabetes (6, 8, and 9 percent, respectively), and systemic hypertension (23, 33, and 34 percent, respectively)
Patient demographics — Most patients are diagnosed with NAFLD in their 40s or 50s . • Studies vary with regard to the sex distribution of NAFLD, with some suggesting it is more common in women and others suggesting it is more common in men. • A higher prevalence of hepatic steatosis in Hispanics (45 percent) compared with whites (33 percent) or blacks (24 percent) .
Association with other disorders — Patients with NAFLD (particularly those with NASH) often have one or more components of the metabolic syndrome . 1)Obesity 2)Systemic hypertension 3)Dyslipidemia 4)Insulin resistance or overt diabetes
NAFLD may be independently associated with cardiovascular disease. • There are also data that suggest NAFLD is associated with • cholecystectomy • Polycystic ovary syndrome • hypothyroidism • obstructive sleep apnea • hypopituitarism • hypogonadism
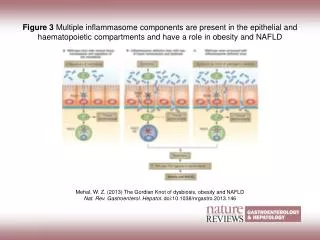
PATHOGENESIS — The pathogenesis of nonalcoholic fatty liver disease has not been fully elucidated. • The most widely supported theory implicates insulin resistance as the key mechanism leading to hepatic steatosis, and perhaps also to steatohepatitis. • Others have proposed that a "second hit", or additional oxidative injury, is required to manifest the necroinflammatory component of steatohepatitis.
CLINICAL MANIFESTATIONS : • Most patients are asymptomatic • Although some patients with nonalcoholic steatohepatitis(NASH) may complain of fatigue, malaise, and vague right upper abdominal discomfort . • laboratory testing revealed normal or elevated liver aminotransferases • Hepatic steatosiswas detected incidentally on abdominal imaging.
Physical findings: Hepatomegaly Among those with NAFLD, 5 percent had hepatomegaly. • Patients who have developed cirrhosis may have stigmata of chronic liver disease (eg, palmar erythema, spider angiomata, ascites).
Laboratory findings — • Mild or moderate elevations in the aspartate aminotransferase (AST) and alanine aminotransferase (ALT) , although normal aminotransferase levels do not exclude NAFLD. • The alkaline phosphatase may be elevated to two to three times the upper limit of normal. • Serum albumin and bilirubin levels are typically within the normal range, but may be abnormal in patients who have developed cirrhosis. • Other laboratory abnormalities that may be seen in patients who have developed cirrhosis include a prolonged prothrombin time, thrombocytopenia, and neutropenia.
There is evidence that a serum ferritin greater than 1.5 times the upper limit of normal in patients with NAFLD is associated: • 1) With a higher nonalcoholic fatty liver disease activity score (and thus, NASH) • 2) With advanced hepatic fibrosis . • Patients with NAFLD may also have positive serum autoantibodies (antinuclear antigen, antismooth muscle antibody), though the significance of these findings is unclear
Radiographic findings — Radiographic findings in patients with NAFLD include: • Increased echogenicity on ultrasound • Decreased hepatic attenuation on CT • An increased fat signal on magnetic resonance imaging (MRI).
DIAGNOSIS — The diagnosis of nonalcoholic fatty liver disease (NAFLD) requires all of the following : 1)Demonstration of hepatic steatosis by imaging or biopsy 2)Exclusion of significant alcohol consumption 3)Exclusion of other causes of hepatic steatosis
Laboratory tests — • The serum aminotransferase and ferritin levels, are often abnormal in NAFLD. • However, these abnormalities are neither required nor sufficient for making the diagnosis
Rule out other disorders — Differentiating NAFLD from the other items in the differential diagnosis begins: • With a thorough history to identify potential causes such as significant alcohol use, starvation, medication use, and pregnancy-related hepatic steatosis.
We obtain the following tests in all patients: ●Anti-hepatitis C virus antibody. ●Hepatitis A IgG. ●Hepatitis B surface antigen, surface antibody, and core antibody. ●Plasma iron, ferritin, and total iron binding capacity. ●Serum gammaglobulin level, antinuclear antibody, antismooth muscle antibody, and anti-liver/kidney microsomal antibody-1 (see "Autoimmune hepatitis: Clinical manifestations and diagnosis", section on 'Diagnosis'). • Other disorders that should be considered based upon the patient's history, associated symptoms, and family history include Wilson disease, thyroid disorders, celiac disease, alpha-1 antitrypsin deficiency, HELLP, and Budd-Chiari syndrome.
Radiographic examinations — Various radiologic methods can detect NAFLD,but no imaging modality is able to differentiate between the histologic subtypes of nonalcoholic fatty liver (NAFL) and nonalcoholic steatohepatitis (NASH) . First imaging is to obtain an ultrasound. However, computed tomography (CT) and magnetic resonance imaging (MRI) can also detect hepatic steatosis.
We consider a radiographic diagnosis to be sufficient for diagnosing NAFLD if all of the following conditions are met: 1)Radiographic imaging is consistent with fatty infiltration 2)Other causes for the patient's liver disease have been excluded 3)The patient does not have signs or symptoms cirrhosis 4)The patient is not at high risk for advanced fibrosis or cirrhosis (eg, a younger patient who does not have diabetes and has a normal serum ferritin is at lower risk for having fibrosis or cirrhosis) • If these criteria are not met, patients will typically require a liver biopsy to make the diagnosis or to assess the degree of liver injury.
Ultrasound — hyperechoic texture or a bright liver because of diffuse fatty infiltration • The sensitivity and specificity for ultrasound were 85 and 94 percent, respectively, when using liver biopsy as the gold standard . • However, the sensitivity appears to be decreased in patients who are morbidly obese.
CT, MRI — Both CT and MRI can identify steatosis but are not sufficiently sensitive to detect inflammation or fibrosis . • The sensitivities of noncontrast CT, contrast-enhanced CT, and MRI for detecting hepatic steatosis were 33, 50, and 88 percent, respectively. The specificities were 100, 83, and 63 percent, respectively. • In addition, the accuracy of noncontrast CT fell with increasing body mass index.
Role of liver biopsy The only way to 1) Definitively confirm or exclude the diagnosis of NASH 2) Determine disease severity is with a liver biopsy
Which patients to biopsy Specifically, we obtain a biopsy if the patient: 1)Has peripheral stigmata of chronic liver disease (suggestive of cirrhosis) 2)Has a serum ferritin >1.5 times the upper limit of normal (suggestive of NASH and advanced fibrosis) 3)Is >45 years of age with associated obesity or diabetes (increased risk of advanced fibrosis)
Histologic findings • The minimum criterion for a histologic diagnosis of NAFLD is >5 percent steatotic hepatocytes in a liver tissue section. • Nonalcoholic fatty liver can be distinguished from NASH based on histologic findings. NAFL is present when the liver biopsy shows any of the following : 1)Steatosis alone. 2)Steatosis with lobular or portal inflammation, without hepatocyte ballooning. 3)Steatosis with hepatocyte ballooning but without inflammation
The histologic diagnosis of NASH requires: • The presence of hepatic steatosis in association with hepatocyte ballooning degeneration and hepatic lobular inflammation (typically in acinar zone 3) . Fibrosis is not a required diagnostic feature, but may be seen.
DIFFERENTIAL DIAGNOSIS ●Alcoholic liver disease ●Hepatitis C (particularly genotype 3) ●Wilson disease ●Lipodystrophy ●Starvation ●Parenteral nutrition ●Abetalipoproteinemia ●Medications (amiodarone, methotrexate, tamoxifen, glucocorticoids, valproate, anti-retroviral agents for HIV) ●Reye syndrome ●Acute fatty liver of pregnancy ●HELLP (hemolytic anemia, elevated liver enzymes, low platelet count) syndrome ●Inborn errors of metabolism (LCAT deficiency, cholesterol ester storage disease, Wolman disease)
Significant alcohol consumption — Several definitions have been proposed for what constitutes significant alcohol consumption . • We define significant alcohol consumption as an average consumption of >210 grams of alcohol per week in men or >140 grams of alcohol per week in women over at least a two-year period, a definition that is consistent with a 2012 joint guideline from the American Gastroenterological Association, the American Association for the Study of Liver Diseases, and the American College of Gastroenterology(AGA,AASLD,ACG).
SCREENING — Currently, the American Association for the Study of Liver Diseases guidelines do not recommend screening because: 1) There are uncertainties around which diagnostic test to use (since liver enzyme levels may be normal in patients with NAFLD) 2) How to treat NAFLD if discovered 3) Whether screening is cost-effective
2)Natural history and management of nonalcoholic fatty liver disease in adults
NATURAL HISTORY — Patients with nonalcoholic fatty liver disease (NAFLD) may eventually develop cirrhosis. • Among patients with cryptogenic cirrhosis, up to 70 percent have risk factors for NAFLD.
Risk factors for progression: • One of the most important risk factors is histologic evidence of hepatic inflammation.
Factors that have been associated with disease progression or advanced fibrosis include in other studies include: ●Older age ●Diabetes mellitus ●Elevated serum aminotransferases (≥2 times the upper limit of normal in one study) ●Presence of ballooning degeneration plus Mallory hyaline or fibrosis on biopsy ●Body mass index (BMI) ≥28 kg/m2 [23] ●Higher visceral adiposity index, which takes into account waist circumference, BMI, triglycerides, and high-density lipoprotein level ●Coffee consumption has been associated with a lower risk of progression
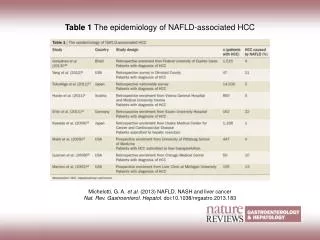
Hepatocellular carcinoma — Hepatocellular carcinoma (HCC) is associated with cirrhosis due to NAFLD. • The risk of HCC among those with cirrhosis ranged from 2.4 percent over seven years to 12.8 percent over three years • Recurrence following liver transplantation — Recurrence of NAFLD has been reported following liver transplantation .
Mortality — Cardiovascular disease is the most common cause of death among patients with NAFLD, though patients with NASH are at increased risk for liver-related death compared with patients without NASH . • Whether patients with NAFLD have increased overall mortality rates compared with the general population is not clear.
MANAGEMENT • General approach to the patient — Multiple therapies have been investigated for the treatment of nonalcoholic fatty liver disease (NAFLD). • Weight loss is the only therapy with reasonable evidence suggesting it is beneficial and safe.
We recommend the following approach in patients with nonalcoholic fatty liver (NAFL) or NASH: 1)Weight loss for patients who are overweight or obese: Options to promote weight loss include lifestyle modifications and, for patients who are candidates, bariatric surgery. A reasonable goal for many patients is to lose 0.5 to 1 kg/week (1 to 2 lb/week). Pharmacologic therapy can be used to aid with weight loss in patients who fail to achieve weight loss goals through diet and exercise alone.
2)Hepatitis A and B vaccinations should be given to patients without serologic evidence of immunity. • Additional vaccines recommended for patients with chronic liver disease include pneumococcal vaccination and standard immunizations recommended for the population in general (eg, influenza, diphtheria, tetanus boosters) (figure 1 and figure 2).
3)Treatment of risk factors for cardiovascular disease: Patients with NAFLD are at increased risk for cardiovascular disease and often have multiple cardiovascular disease risk factors. Management of patients with NAFLD includes: • Optimization of blood pressure, • Glucose control in patients with diabetes and • Treatment of hyperlipidemia. Statin therapy has been shown to be safe in patients with NAFLD.
4)In general, we do not suggest using pharmacologic agents (eg, vitamin E, pioglitazone) solely for the treatment of NAFLD. • However, we do suggest vitamin E at a dose of 400 international units/day for the subset of patients with advanced fibrosis on biopsy who do not have diabetes or coronary artery disease.
5)We suggest that patients with NAFLD avoid all alcohol consumption. Heavy alcohol use is associated with disease progression among patients with NAFLD.
Insulin-sensitizing agents — Whereas the thiazolidinediones have been shown to improve histologic parameters in patients with NASH, metformin has not. • However, thiazolidinediones are associated with significant side effects and are thus not routinely used for the treatment of NASH.